

AAPM task group report 135.B: Quality assurance for robotic radiosurgery
- PMID: 39453412
- PMCID: PMC11700000
- DOI: 10.1002/mp.17478
AAPM task group report 135.B: Quality assurance for robotic radiosurgery
Abstract
AAPM Task Group Report 135.B covers new technology components that have been added to an established radiosurgery platform and updates the components that were not well covered in the previous report. Considering the current state of the platform, this task group (TG) is a combination of a foundational task group to establish the basis for new processes/technology and an educational task group updating guidelines on the established components of the platform. Because the technology discussed in this document has a relatively small user base compared to C-arm isocentric linacs, the authors chose to emphasize the educational components to assist medical physicists who are new to the technology and have not had the opportunity to receive in-depth vendor training at the time of reading this report. The TG has developed codes of practice, introduced QA, and developed guidelines which are generally expected to become enduring practice. This report makes prescriptive recommendations as there has not been enough longitudinal experience with some of the new technical components to develop a data-based risk analysis.
Keywords: image guided SBRT; image guided SRS; robotic radio‐surgery.
© 2024 The Author(s). Medical Physics published by Wiley Periodicals LLC on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The Chair of the AAPM Task Group Report 135.B has reviewed the required Conflict of Interest statement on file or each member of AAPM Task Group Report 135.B and determined that disclosure of potential Conflicts of Interest is an adequate management plan.
The members of AAPM Task Group Report 135.B listed below attest that they have no potential Conflicts of Interest related to the subject matter or materials presented in this document: Lei Wang, Anand Prabhu, Ellen Wilcox, Jun Yang, Christoph Fuerweger, Jeffrey Garrett, David Taylor, Sonja Dieterich.
The members of AAPM Task Group Report 135.B listed below disclose the following potential Conflict(s) of Interest related to subject matter or materials presented in this document: Alan Cohen, Matt Noll, Martina Descovich.
Alan Cohen worked as a medical physicist at Accuray Inc. between November 2006 to June 2016. Matt Noll is currently the senior physics manager at Accuray Inc. Martina Descovich served as a member of the CyberKnife and Radixact clinical advisory boards in 2017–2018
Figures
References
-
- Dieterich S, Cavedon C, Chuang CF, et al. Report of AAPM TG 135: quality assurance for robotic radiosurgery [published online ahead of print 2011/08/06]. Med Phys. 2011;38(6):2914‐2936. - PubMed
-
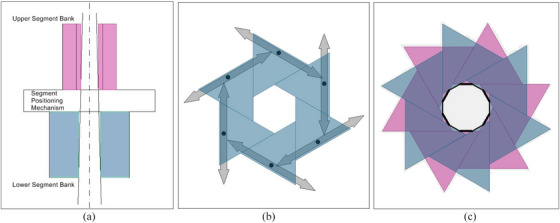
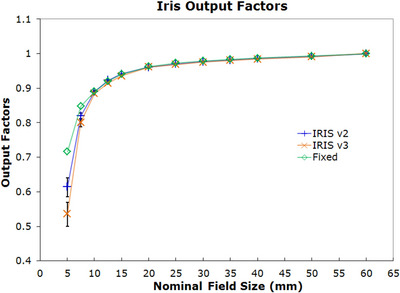
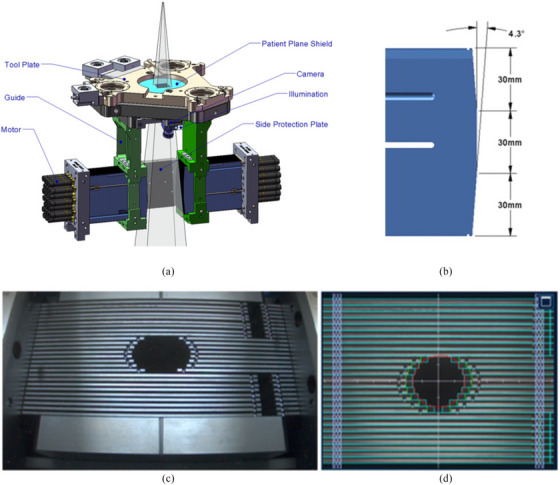
- Echner GG, Kilby W, Lee M, et al. The design, physical properties and clinical utility of an iris collimator for robotic radiosurgery [published online ahead of print 2009/08/19]. Phys Med Biol. 2009;54(18):5359‐5380. - PubMed
-
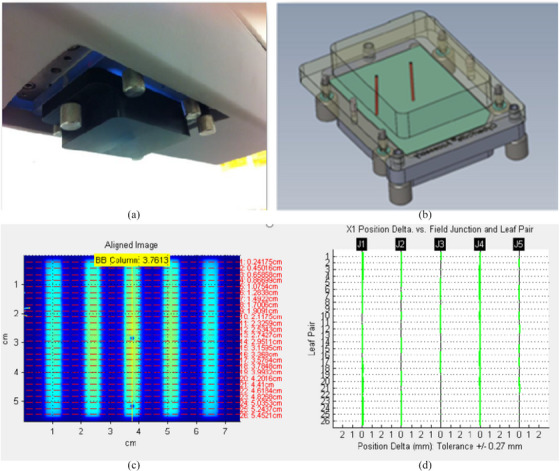
- Fürweger C, Prins P, Coskan H, Heijmen BJ. Characteristics and performance of the first commercial multileaf collimator for a robotic radiosurgery system. Med Phys. 2016;43(5):2063‐2071. - PubMed
-
- Asmerom G, Bourne D, Chappelow J, et al. The design and physical characterization of a multileaf collimator for robotic radiosurgery. Biomed Phys Eng Express. 2016;2(1):017003.
-
- Benjamin P, Fahimian LW. Introduction to CyberKnife® Technology. In: Steven D. Chang AV, eds. CyberKnife Stereotactic Radiosurgery. Nova Science Publishers, Inc.; 2014:1‐12.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
