

It takes a village: A pilot cross-randomized trial to enhance pregnancy care and support in northern Ghana
- PMID: 39453695
- PMCID: PMC11506688
- DOI: 10.7189/jogh.14.04217
It takes a village: A pilot cross-randomized trial to enhance pregnancy care and support in northern Ghana
Abstract
Background: Maternal mortality remains a challenge in Ghana, where 263 women per 100 000 live births die during pregnancy or childbirth. Barriers to reaching the recommended antenatal care (ANC) include poor access to quality health care, cultural factors, and lack of support for pregnant women.
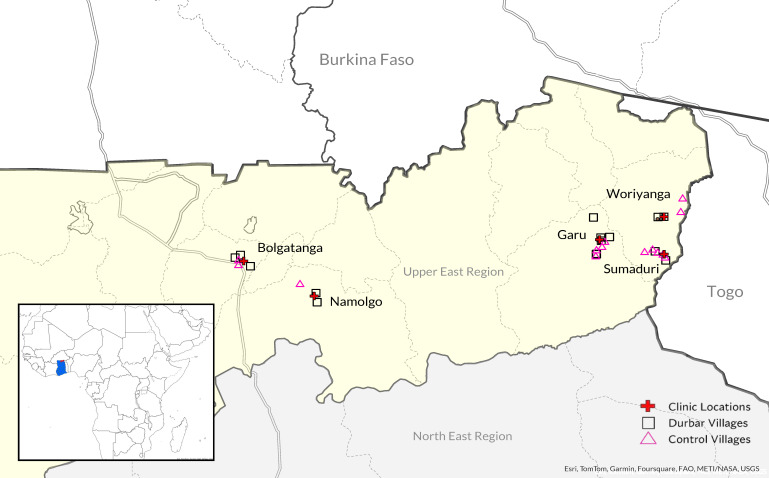
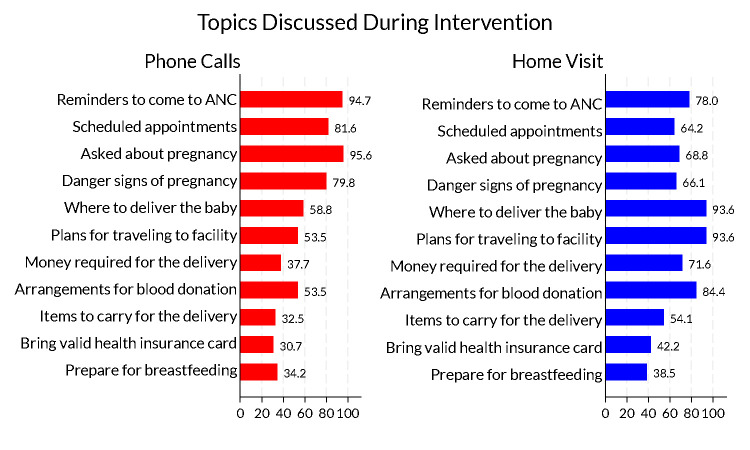
Methods: We piloted two cross-randomized interventions: durbars, or local community meetings that incorporated education about ANC and supporting pregnant women, and an enhanced ANC model that added phone calls and a home visit to standard care. The study took place in 30 villages in the Upper East Region of Ghana between August 2021 and November 2022.
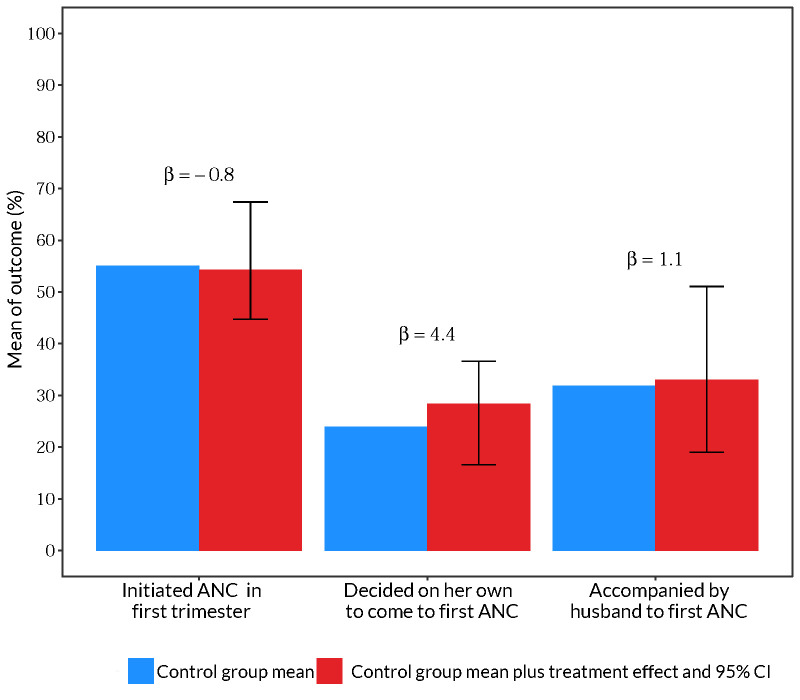
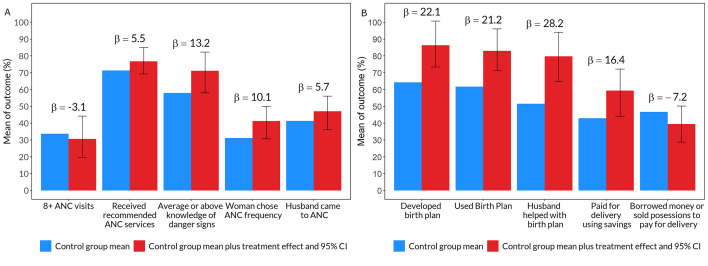
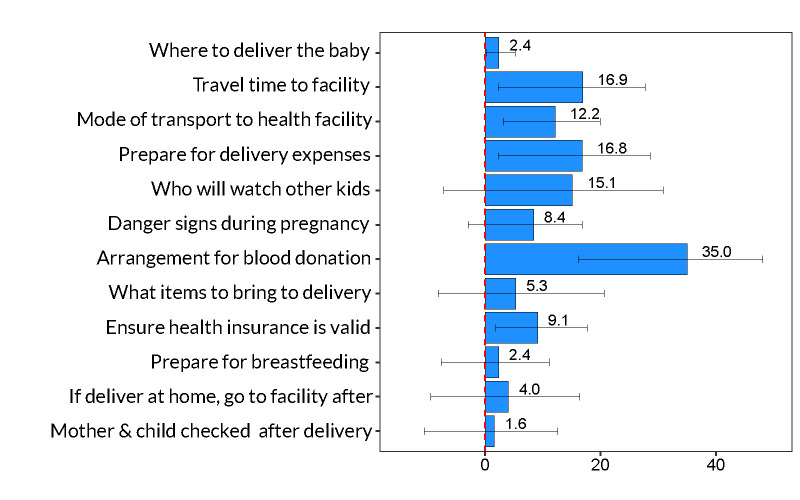
Results: We tracked 277 women during pregnancy, with 120 women randomly assigned to the enhanced ANC intervention and 142 women living in villages randomized to the durbar intervention. Women who were randomized to the enhanced ANC intervention were 13.2 percentage points (pp) (95% confidence interval (CI) = 0.1, 24.3) more likely to have average or above average knowledge of pregnancy danger signs, 22.1 pp (95% CI = 9.1, 36.5) more likely to have a birth plan, 28.2 pp (95% CI = 13.0, 42.4) more likely to prepare the plan with their partners, and 16.4 pp (95% CI = 0.9, 29.3) more likely to pay for delivery with funds set aside in birth plan. They were also 35 pp (95% CI = 16.1, 48.1) more likely to make blood donor arrangements than control women who made birth plans. We found no impact of the durbar intervention on study outcomes.
Conclusions: Evidence from this pilot suggests that interventions that increase interactions between health providers and pregnant women outside of the health facility may substantially improve women's experience during pregnancy and maternal health outcomes. Providing structured ways for men to get engaged in ANC increased their involvement. Although we found no evidence the community meetings improved study outcomes, larger studies with repeated meetings and community-wide surveys are needed to make causal conclusions.
Registration: American Economic Association RCT Registry: 10360; ISCRNT: ISRCTN95961119.
Copyright © 2024 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interest: The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Figures
Similar articles
-
Boosting antenatal care attendance and number of hospital deliveries among pregnant women in rural communities: a community initiative in Ghana based on mobile phones applications and portable ultrasound scans.BMC Pregnancy Childbirth. 2016 Jun 14;16(1):141. doi: 10.1186/s12884-016-0888-x. BMC Pregnancy Childbirth. 2016. PMID: 27301244 Free PMC article.
-
The power of peers: an effectiveness evaluation of a cluster-controlled trial of group antenatal care in rural Nepal.Reprod Health. 2019 Oct 22;16(1):150. doi: 10.1186/s12978-019-0820-8. Reprod Health. 2019. PMID: 31640770 Free PMC article.
-
Factors associated with utilization of skilled service delivery among women in rural Northern Ghana: a cross sectional study.BMC Pregnancy Childbirth. 2017 May 31;17(1):159. doi: 10.1186/s12884-017-1344-2. BMC Pregnancy Childbirth. 2017. PMID: 28566088 Free PMC article.
-
Evaluation of a package of continuum of care interventions for improved maternal, newborn, and child health outcomes and service coverage in Ghana: A cluster-randomized trial.PLoS Med. 2021 Jun 25;18(6):e1003663. doi: 10.1371/journal.pmed.1003663. eCollection 2021 Jun. PLoS Med. 2021. PMID: 34170904 Free PMC article. Clinical Trial.
-
Quality of antenatal care services received by women of reproductive age prior to delivery in selected public health facilities in the northern zone of Ghana.BMC Health Serv Res. 2024 Sep 13;24(1):1063. doi: 10.1186/s12913-024-11491-1. BMC Health Serv Res. 2024. PMID: 39272145 Free PMC article.
References
-
- World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva, Switzerland: World Health Organization; 2016. Available: https://www.who.int/publications/i/item/9789241549912. Accessed: 9 October 2024.
-
- World Health Organization. WHO recommendations on postnatal care of the mother and newborn. Geneva, Switzerland: World Health Organization; 2016. Available: https://www.who.int/publications/i/item/9789241506649. Accessed: 9 October 2024.
-
- World Health Organization. Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva, Switzerland: World Health Organization; 2016. Available: http://documents1.worldbank.org/curated/en/793971568908763231/pdf/Trends.... Accessed: 9 October 2024.
-
- United Nations. The 17 Goals: Sustainable Development. 2024. Available: https://sdgs.un.org/goals/goal3. Accessed: 9 October 2024.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
