

Yellow fever disease severity and endothelial dysfunction are associated with elevated serum levels of viral NS1 protein and syndecan-1
- PMID: 39454515
- PMCID: PMC11539239
- DOI: 10.1016/j.ebiom.2024.105409
Yellow fever disease severity and endothelial dysfunction are associated with elevated serum levels of viral NS1 protein and syndecan-1
Abstract
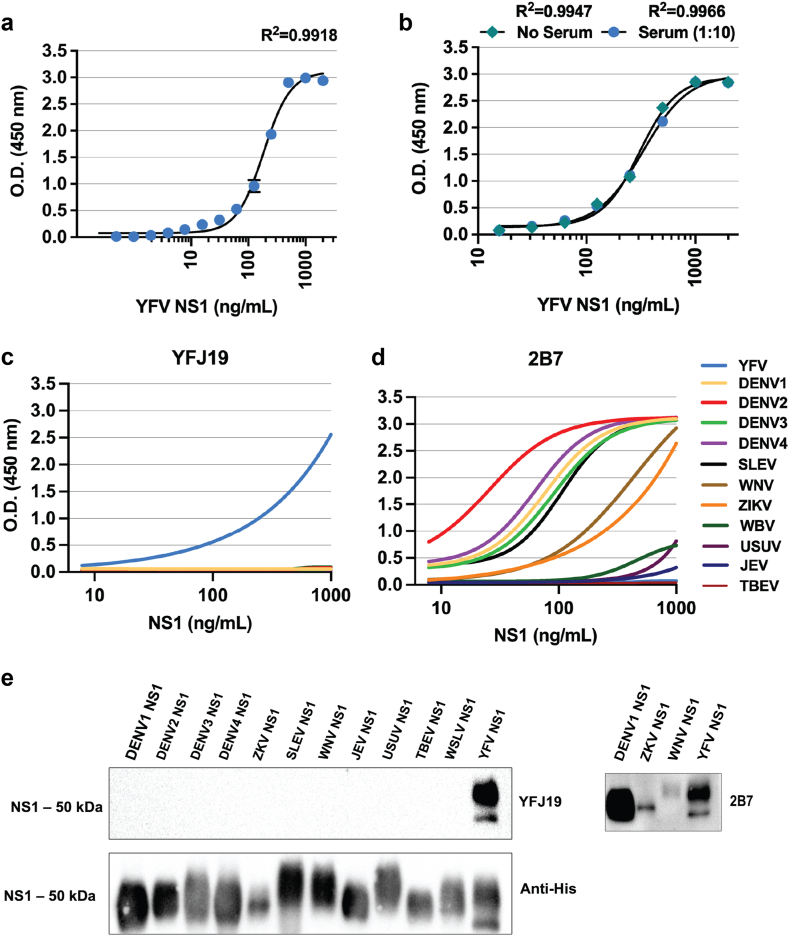
Background: Yellow fever virus (YFV) infections are a major global disease concern with high mortality in humans, and as such it is critical to identify clinical correlates of disease severity. While nonstructural protein 1 (NS1) of the related dengue virus is implicated in contributing to vascular leak, little is known about the role of YFV NS1 in severe YF and mechanisms of vascular dysfunction in YFV infections.
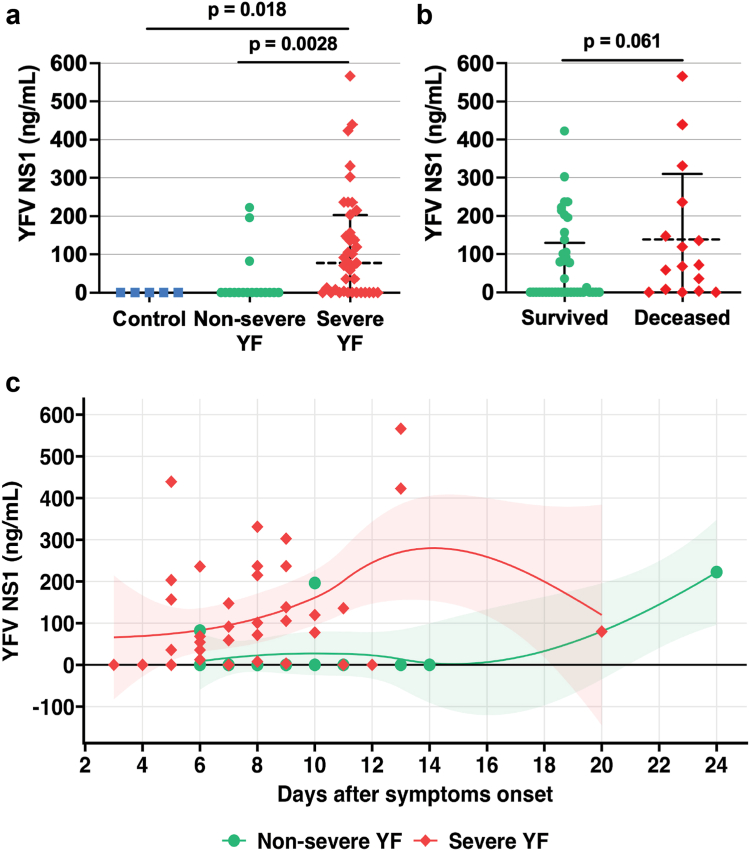
Methods: Using serum samples from laboratory-confirmed YF patients with severe (n = 39) or non-severe (n = 18) disease in a well-defined hospital observational cohort in Brazil, plus samples from healthy uninfected controls (n = 11), we investigated factors associated with disease severity and endothelial dysfunction.
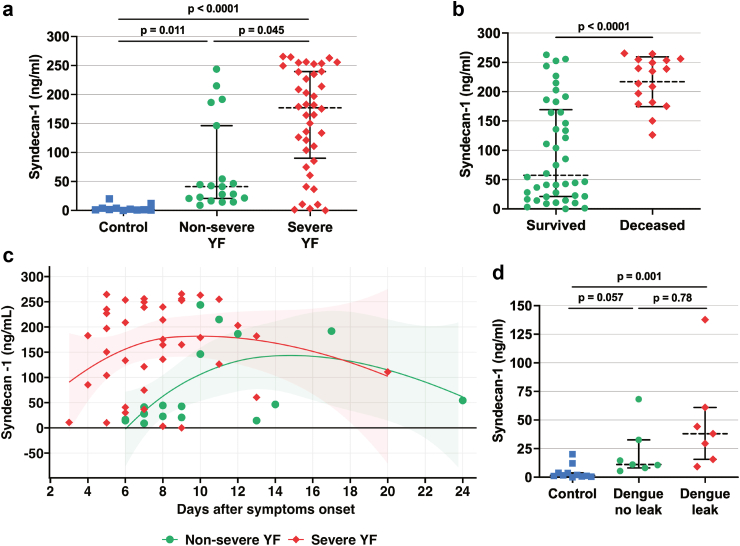
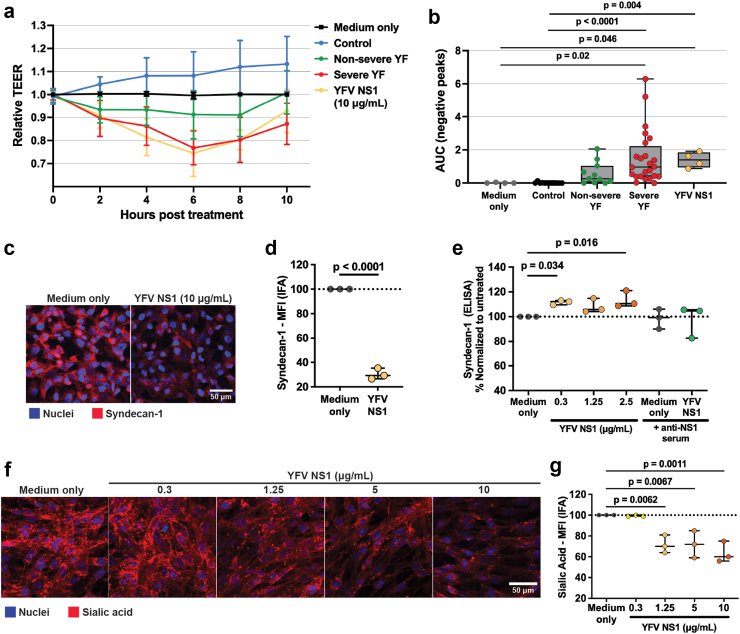
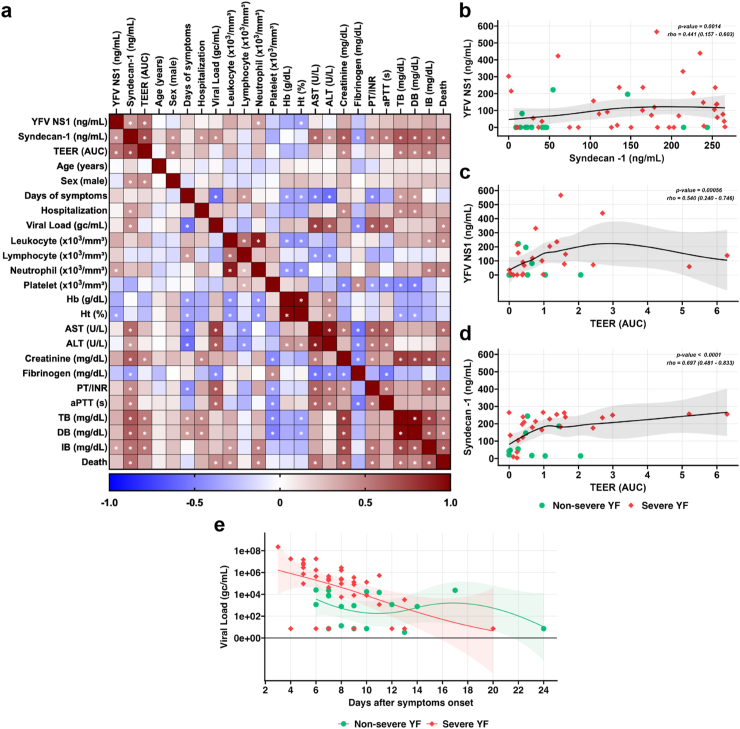
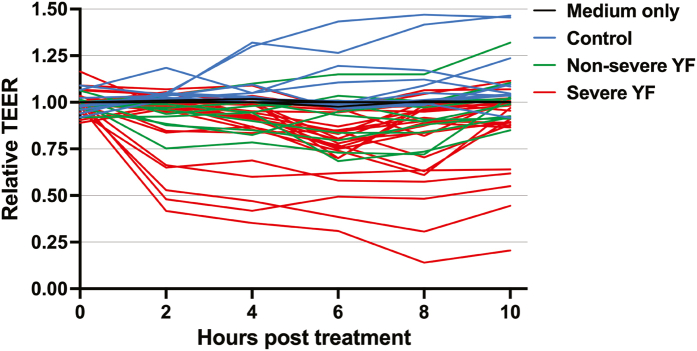
Findings: We found significantly increased levels of NS1, as well as syndecan-1, a marker of vascular leak, in serum from severe YF as compared to non-severe YF or control groups. We also showed that hyperpermeability of endothelial cell monolayers treated with serum from severe YF patients was significantly higher compared to non-severe YF and control groups, as measured by transendothelial electrical resistance (TEER). Further, we demonstrated that YFV NS1 induces shedding of syndecan-1 from the surface of human endothelial cells. Notably, YFV NS1 serum levels significantly correlated with syndecan-1 serum levels, TEER values, and signs of disease severity. Syndecan-1 levels also significantly correlated with clinical laboratory parameters of disease severity, viral load, hospitalization, and death.
Interpretation: This study provides further evidence for endothelial dysfunction as a mechanism of YF pathogenesis in humans and suggests serum quantification of YFV NS1 and syndecan-1 as valuable tools for disease diagnosis and/or prognosis.
Funding: This work was supported by the US NIH and FAPESP.
Keywords: Endothelial dysfunction; NS1; Pathogenesis; Syndecan-1; Yellow fever.
Copyright © 2024 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no conflict of interests.
Figures
Update of
-
Yellow fever disease severity and endothelial dysfunction are associated with elevated serum levels of viral NS1 protein and syndecan-1.medRxiv [Preprint]. 2023 Jun 30:2023.06.29.23292053. doi: 10.1101/2023.06.29.23292053. medRxiv. 2023. Update in: EBioMedicine. 2024 Nov;109:105409. doi: 10.1016/j.ebiom.2024.105409. PMID: 37425955 Free PMC article. Updated. Preprint.
References
-
- Kallas E.G., D'Elia Zanella L.G.F.A.B., Moreira C.H.V., et al. Predictors of mortality in patients with yellow fever: an observational cohort study. Lancet Infect Dis. 2019;19:750–758. - PubMed
-
- Libraty D.H., Young P.R., Pickering D., et al. High circulating levels of the dengue virus nonstructural protein NS1 early in dengue illness correlate with the development of dengue hemorrhagic fever. J Infect Dis. 2002;186:1165–1168. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
