

Continuous Blood Pressure Indices During the First 72 Hours and Functional Outcome in Patients with Spontaneous Intracerebral Hemorrhage
- PMID: 39455525
- PMCID: PMC12137446
- DOI: 10.1007/s12028-024-02146-4
Continuous Blood Pressure Indices During the First 72 Hours and Functional Outcome in Patients with Spontaneous Intracerebral Hemorrhage
Abstract
Background: Management of intracerebral hemorrhage (ICH) is challenged by limited therapeutic options and a complex relationship between blood pressure (BP) dynamics, especially BP variability (BPV) and ICH outcome.
Methods: In an exploratory analysis of prospectively collected data on consecutive patients with nontraumatic ICH between 2015 and 2020, continuous BP accessed via an arterial line extracted from the Intellispace Critical Care and Anesthesia information system (Philips Healthcare) was analyzed over the first 72 h post admission. Arterial lines were used as part of standard clinical practice in the intensive care, ensuring high fidelity and real-time data essential for acute care settings. BPV was assessed through successive variation (SV), standard deviation (SD), and coefficient of variation using all available BP measurements. Multivariate regression models were applied to evaluate the association between BPV indices and functional outcome at 3 months.
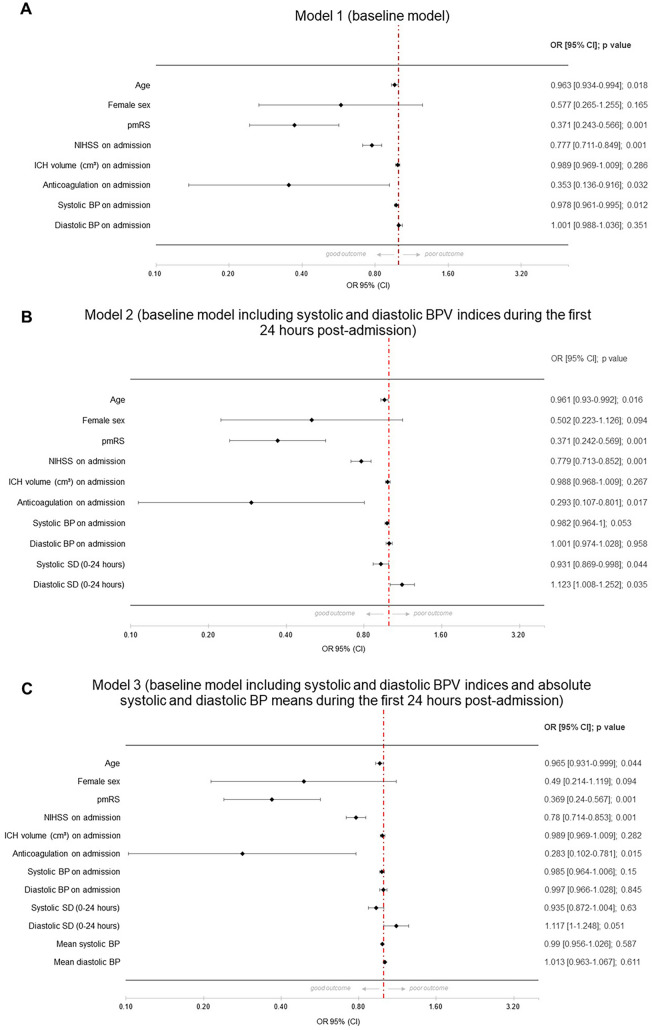
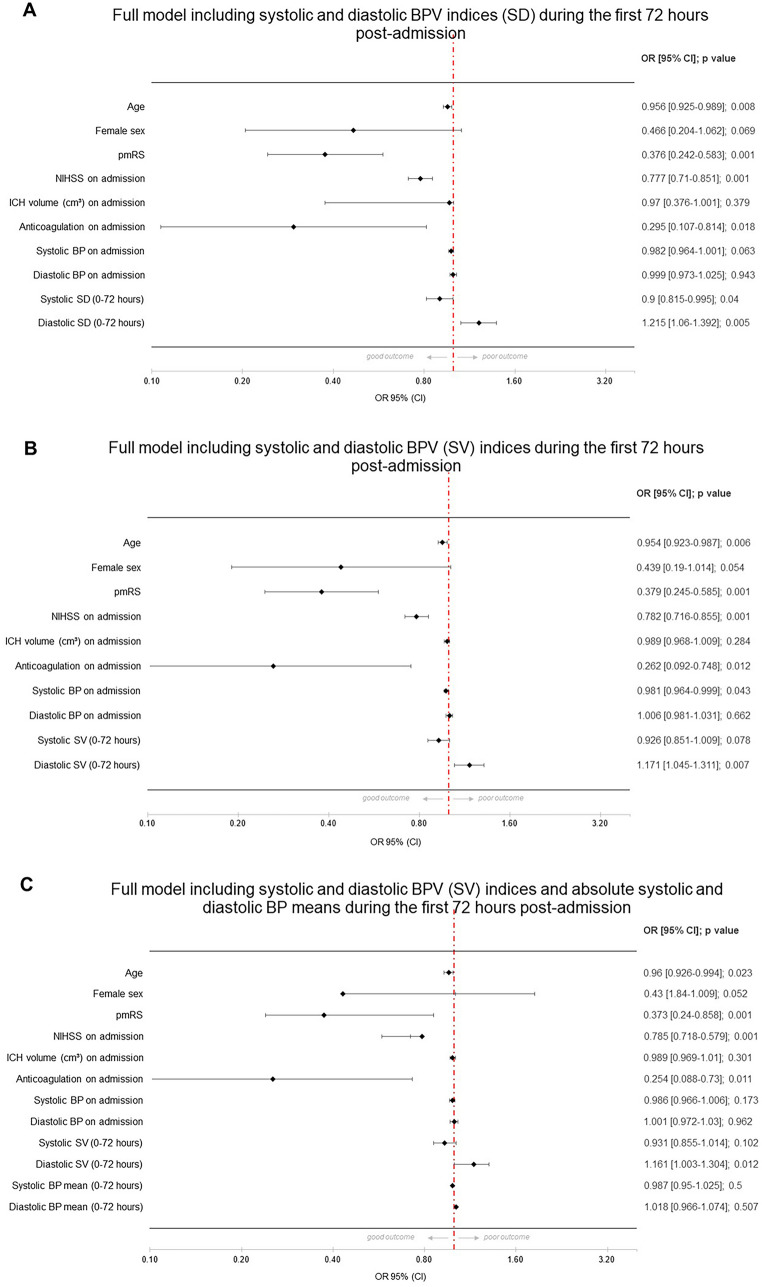
Results: Among 261 patients (mean age 69.6 ± 15.2 years, 47.9% female, median National Institutes of Health Stroke Scale [NIHSS] score 6 [interquartile range 2-12]) analyzed, lower systolic BP upon admission (< 140 mm Hg) and lower systolic BPV were significantly associated with favorable outcome, whereas higher diastolic BPV correlated with improved outcomes. In the multivariate analysis, diastolic BPV (SD, SV) within the first 72 h post admission emerged as an independent predictor of good functional outcome (modified Rankin Scale score < 3; odds ratio 1.123, 95% confidence interval CI 1.008-1.184, p = 0.035), whereas systolic BPV (SD) showed a negative association. Patients with better outcomes also exhibited distinct clinical characteristics, including younger age, lower median NIHSS scores, and less prevalence of anticoagulation therapy upon admission.
Conclusions: This study shows the prognostic value of BPV in the acute phase of ICH. Lower systolic BPV (SD) and higher diastolic BPV (SD, SV) were associated with better functional outcomes, challenging traditional BP management strategies. These findings might help to tailor a personalized BP management in ICH.
Keywords: Blood pressure variability; Functional outcome; Intracerebral hemorrhage; Mortality.
© 2024. The Author(s).
Conflict of interest statement
Conflicts of interest: Vasileios Siokas is supported with a scholarship from the Hellenic Neurological Society, which played no role in the design of the study, collection and/or interpretation of data, or writing of the article. Katharina Feil received speakers’ honoraria/consulting fees from, AstraZeneca and BMS/Pfizer (all outside the submitted work). Ethical Approval: Due to the clinic-wide consent regarding the use of routine treatment data for research purposes, the individual informed consent from the participants was waived (protocol number 545/2022BO2).
Figures

References
-
- Rothwell PM, Coull AJ, Giles MF, Howard SC, Silver LE, Bull LM, et al. Change in stroke incidence, mortality, case-fatality, severity, and risk factors in Oxfordshire, UK from 1981 to 2004 (Oxford vascular study). Lancet. 2004;363(9425):1925–33. - PubMed
-
- Greenberg SM, Ziai WC, Cordonnier C, Dowlatshahi D, Francis B, Goldstein JN, et al. Guideline for the management of patients with spontaneous intracerebral hemorrhage: a guideline from the American heart association/American stroke association. Stroke. 2022;53(7):e282–361. - PubMed
-
- Ovbiagele B, Goldstein LB, Higashida RT, Howard VJ, Johnston SC, Khavjou OA, et al. Forecasting the future of stroke in the United States: a policy statement from the American heart association and American stroke association. Stroke. 2013;44(8):2361–75. - PubMed
-
- Gross BA, Jankowitz BT, Friedlander RM. Cerebral intraparenchymal hemorrhage: a review. JAMA. 2019;321(13):1295–303. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
