

Development of a nomogram-based model incorporating radiomic features from follow-up longitudinal lung CT images to distinguish invasive adenocarcinoma from benign lesions: a retrospective study
- PMID: 39455958
- PMCID: PMC11515265
- DOI: 10.1186/s12890-024-03360-8
Development of a nomogram-based model incorporating radiomic features from follow-up longitudinal lung CT images to distinguish invasive adenocarcinoma from benign lesions: a retrospective study
Abstract
Purpose: To develop and validate a radiomic model for differentiating pulmonary invasive adenocarcinomas from benign lesions based on follow-up longitudinal CT images.
Methods: This is a retrospective study including 336 patients (161 with invasive adenocarcinomas and 175 with benign lesions) who underwent baseline (T0) and follow-up (T1) CT scans from January 2016 to June 2022. The patients were randomized in a 7:3 ratio into training and test sets. Radiomic features were extracted from lesion volumes of interest on longitudinal CT images at T0 and T1. Differences in radiomic features between T1 and T0 were defined as delta-radiomic features. Logistic regression was used to build models based on clinicoradiological (CR), T0, T1, and delta radiomic features and compute signatures. Finally, a nomogram based on the CR, T0, T1 and delta signatures was constructed. Model performance was evaluated for calibration, discrimination, and clinical utility.
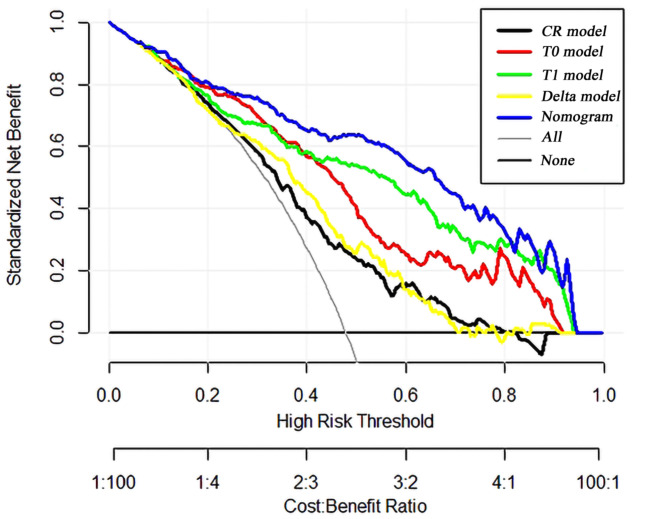
Results: The T1 radiomic model was superior to the other independent models. In the training set, it had an area under the curve (AUC) of 0.858), superior to the CR model (AUC 0.694), the T0 radiomic model (AUC 0.825), and the delta radiomic model (AUC 0.734). In the test set, it had an AUC of 0.817, again outperforming the CR model (AUC 0.578), the T0 radiomic model (AUC 0.789), and the delta radiomic model (AUC 0.647). The nomogram incorporating the CR, T0, T1 and delta signatures showed the best predictive performance in both the training (AUC: 0.906) and test sets (AUC: 0.856), and it exhibited excellent fit with calibration curves. Decision curve analysis provided additional validation of the clinical utility of the nomogram.
Conclusion: A nomogram utilizing radiomic features extracted from longitudinal CT images can enhance the discriminative capability between pulmonary invasive adenocarcinomas and benign lesions.
Keywords: CT image; Identification; Nomogram; Pulmonary nodule; Radiomic.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





Similar articles
-
A combination of radiomic features, clinic characteristics, and serum tumor biomarkers to predict the possibility of the micropapillary/solid component of lung adenocarcinoma.Ther Adv Respir Dis. 2024 Jan-Dec;18:17534666241249168. doi: 10.1177/17534666241249168. Ther Adv Respir Dis. 2024. PMID: 38757628 Free PMC article.
-
Integrative nomogram of intratumoral, peritumoral, and lymph node radiomic features for prediction of lymph node metastasis in cT1N0M0 lung adenocarcinomas.Sci Rep. 2021 May 24;11(1):10829. doi: 10.1038/s41598-021-90367-4. Sci Rep. 2021. PMID: 34031529 Free PMC article.
-
A comparative study to evaluate CT-based semantic and radiomic features in preoperative diagnosis of invasive pulmonary adenocarcinomas manifesting as subsolid nodules.Sci Rep. 2021 Jan 18;11(1):66. doi: 10.1038/s41598-020-79690-4. Sci Rep. 2021. PMID: 33462251 Free PMC article.
-
Radiomic nomograms in CT diagnosis of gall bladder carcinoma: a narrative review.Discov Oncol. 2024 Dec 27;15(1):844. doi: 10.1007/s12672-024-01720-8. Discov Oncol. 2024. PMID: 39730762 Free PMC article. Review.
-
Mastering CT-based radiomic research in lung cancer: a practical guide from study design to critical appraisal.Br J Radiol. 2025 May 1;98(1169):653-668. doi: 10.1093/bjr/tqaf051. Br J Radiol. 2025. PMID: 40100283 Free PMC article. Review.
References
-
- Gould MK, Donington J, Lynch WR, Mazzone PJ, Midthun DE, Wiener RS, et al. Evaluation of individuals with pulmonary nodules: when is it lung cancer? Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):eS93–120. - PMC - PubMed
-
- Callister ME, Baldwin DR, Akram AR, Barnard S, Cane P, British Thoracic Society Standards of Care Committee. British Thoracic Society guidelines for the investigation and management of pulmonary nodules. Thorax. 2015;70(Suppl 2):ii1–54. - PubMed
-
- MacMahon H, Austin JH, Gamsu G, Herold CJ, Jett JR, et al. Fleischner Society. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology. 2005;237(2):395–400. - PubMed
-
- MacMahon H, Naidich DP, Goo JM, Lee KS, Leung ANC, Bankier AA, et al. Guidelines for management of Incidental Pulmonary nodules detected on CT images: from the Fleischner Society 2017. Radiology. 2017l;284(1):228–43. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
