

Intravenous injection versus transhepatic intracholecystic injection of indocyanine green (ICG) to outline biliary tree during laparoscopic cholecystectomy
- PMID: 39455983
- PMCID: PMC11515391
- DOI: 10.1186/s12893-024-02612-y
Intravenous injection versus transhepatic intracholecystic injection of indocyanine green (ICG) to outline biliary tree during laparoscopic cholecystectomy
Abstract
Background: To potentially lessen injuries and associated complications, fluorescence cholangiography has been suggested as a technique for enhancing the visualization and identification of extrahepatic biliary anatomy. The most popular way to administer indocyanine green (ICG) is intravenously, as there is currently little data on ICG injections directly into the gallbladder. In order to visualize extrahepatic biliary anatomy during laparoscopic cholecystectomy (LC), we compared the two different ICG administration techniques. We also examined variations in visualization time, as well as the effectiveness, benefits, and drawbacks of each modality.
Methods: In this prospective randomized clinical study, 60 consecutive adult patients with chronic and acute gallbladder disease were included. Our study conducted from 2022 to 2024 in Surgical Department of Theodor Bilharz Research Institute. Thirty patients underwent LC with intravenous ICG administration (IV-ICG), thirty patients received a direct injection of gallbladder through transhepatic ICG (IC-ICG) and Preoperative, intraoperative, and postoperative patient data were examined.
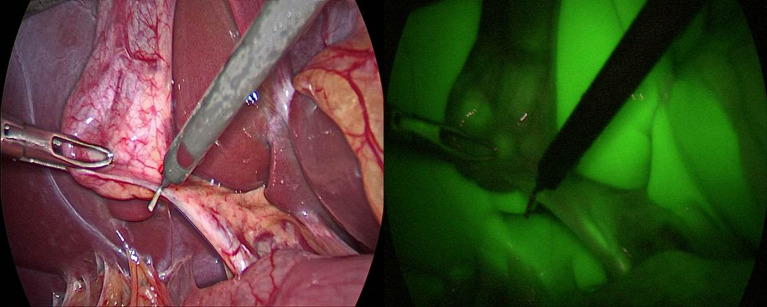
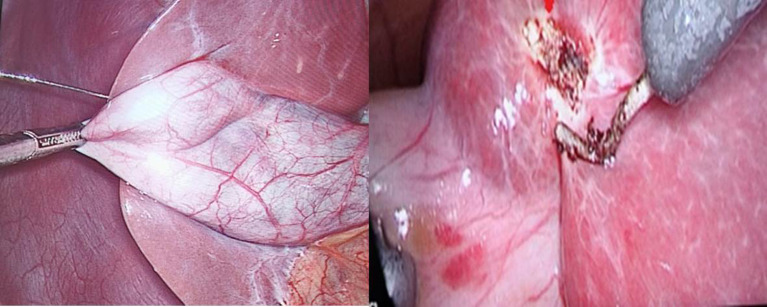
Results: In terms of their perioperative and demographic features, the groups were similar. Without a statistically significant difference, the IV-ICG group's total operating time was less than that of the IC-ICG group (p 0.140). Compared to the transhepatic IC-ICG method, IV-ICG was more accurate in identifying the duodenum and the common hepatic duct (p = 0.029 and p = 0.016, respectively). In the transhepatic IC-ICG and IV-ICG groups, the cystic duct could be identified prior to dissection in 66.6% and 73.3% of cases, respectively, and this increased to 86.6% and 93.3% following dissection. In the transhepatic IC-ICG group, the common bile duct was visible in 93.3% of cases; in the IV-ICG group, it was visible in 90% of cases. Two cases in the IC-ICG group and every case following IV-ICG administration had liver fluorescence (6.6% versus 100%; p < 0.001).
Conclusion: The current study shows that for both administration methods, ICG-fluorescence cholangiography can be useful in identifying the extrahepatic biliary anatomy during Calot's triangle dissection. By avoiding hepatic fluorescence, the transhepatic IC-ICG route can increase the bile duct-to-liver contrast with less expense and no risk of hypersensitivity reactions than the intravenous ICG injection method. We recommend to use both techniques in case of acute cholecystitis with cystic duct obstruction. In cases of liver cirrhosis, we recommend transhepatic IC-ICG as IV-ICG is limited.
Keywords: Common bile duct injury; Fluorescence cholangiography; Indocyanine green; Intracholecystic; Laparoscopic cholecystectomy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Serban D, Socea B, Balasescu SA, Badiu CD, Tudor C, Dascalu AM, Vancea G, Spataru RI, Sabau AD, Sabau D, Tanasescu C. Safety of laparoscopic cholecystectomy for acute cholecystitis in the elderly: a multivariate analysis of risk factors for intra and postoperative complications. Med (Kaunas). 2021;57:230. - PMC - PubMed
-
- Fometescu SG, Costache M, Coveney A, Oprescu SM, Serban D, Savlovschi C. Peritoneal fibrinolytic activity and adhesiogenesis. Chirurgia (Bucur). 2013;108:331–40. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
