

The Importance of Patient Systemic Health Status in High-Grade Chondrosarcoma Prognosis: A National Multicenter Study
- PMID: 39456578
- PMCID: PMC11506449
- DOI: 10.3390/cancers16203484
The Importance of Patient Systemic Health Status in High-Grade Chondrosarcoma Prognosis: A National Multicenter Study
Abstract
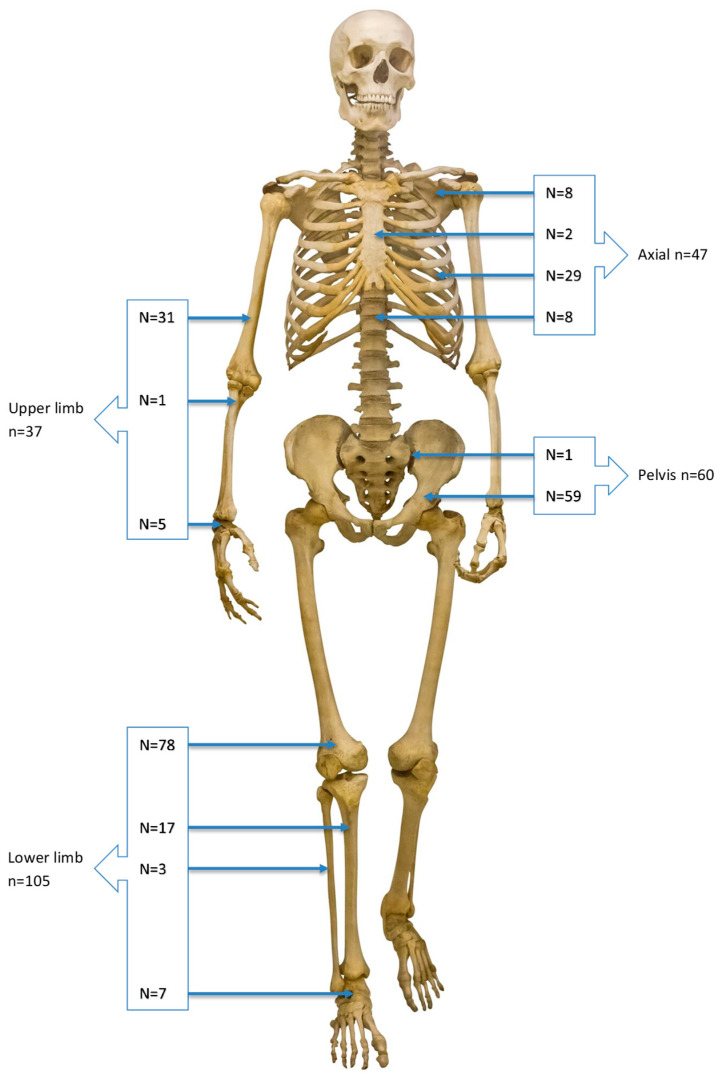
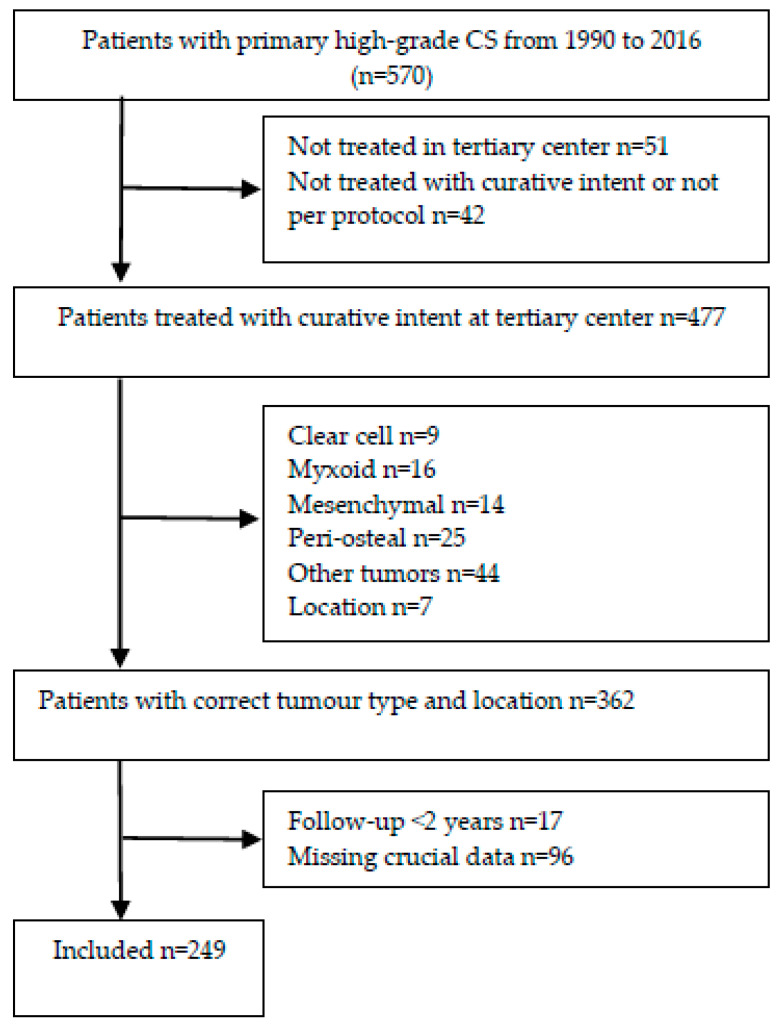
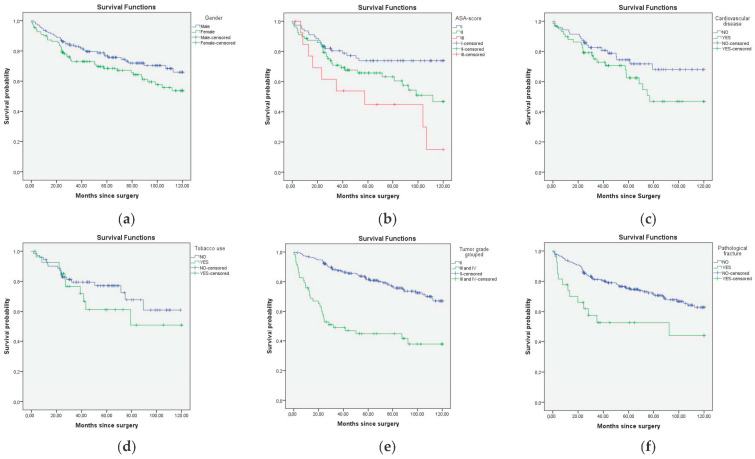
Background: Due to the relatively advanced age and high mortality rate of patients with high-grade chondrosarcoma (CS), it is important to holistically assess patient- and tumor characteristics in multidisciplinary team and shared decision-making with regard to treatment options. While current prognostic models include multiple tumor and treatment characteristics, the only patient characteristics that are commonly included are age and gender. Based on clinical experience, we believe that factors related to patient preoperative systemic health status such as the American Society of Anesthesiologists (ASA) score may be equally important prognostic factors for overall survival (OS). Methods: A retrospective nationwide cohort study was identified from four specialized bone sarcoma centers in The Netherlands. Patients with a primary CS grade II, III, and dedifferentiated CS were eligible. Prognostic factors including age at presentation, gender, ASA score, CVD, tobacco use, BMI, histological tumor grade, tumor size, pathological fracture, presentation after unplanned excision, type of surgery and surgical margin were evaluated. The outcome measure was OS at the time of surgery. The Kaplan-Meier methodology was employed to estimate OS; a log-rank test was used to assess the difference in survival. To study the impact of prognostic factors on OS, a multivariate Cox proportional hazard regression model was estimated. Results: In total, 249 patients were eligible for this study, and 89 were deceased at the end of follow-up. In multivariate analysis, histological grade (HR 2.247, 95% CI 1.334-3.783), ASA score III (HR 2.615, 95% CI 1.145-5.976, vs. ASA I), and age per year (HR: 1.025, 95% CI 1.004-1.045) were negatively associated with OS. No association was found between tobacco use, BMI, gender or cardiovascular disease and OS in this cohort. Pathological fracture and tumor size were only associated with OS in univariate analysis. Conclusions: This multicenter study is the first on sarcomas to include ASA in a prognostic model. Results show that ASA score as a proxy for patients' systemic health status should be included when providing a prognosis for patients with a high-grade primary CS, besides the conventional risk factors such as tumor grade and age. Specifically, severe systemic disease (ASA score III) is a strong negative predictor. Conversely, we found no difference in OS between ASA scores I and II. These findings aid multidisciplinary team and shared decision-making with regard to these complex sarcoma patients that often require life-changing surgeries. Level of Evidence: Prognostic level III. See the instructions for authors for the complete description of levels of evidence.
Keywords: ASA-score; bone malignancies; chondrosarcoma; patient systemic health.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Bertoni F., Bacchini P., Hogendoorn P.C.W. Pathology and Genetics of Tumours of Soft Tissue and Bone. World Health Organization Classification of Tumours; Geneva, Switzerland: 2002. pp. 247–251.
LinkOut - more resources
Full Text Sources
