

Stereotactic Radiosurgery for Intracranial Breast Metastases: A Systematic Review and Meta-Analysis
- PMID: 39456645
- PMCID: PMC11506708
- DOI: 10.3390/cancers16203551
Stereotactic Radiosurgery for Intracranial Breast Metastases: A Systematic Review and Meta-Analysis
Abstract
Background/objectives: To determine the impact of stereotactic radiosurgery on outcomes of metastatic breast cancer with intracranial metastases.
Methods: We systematically searched the PubMed and EMBASE databases for studies published between 1 January 1990 and 1 August 2024. Primary research articles evaluating the outcomes of stereotactic radiosurgery on intracranial metastases from breast cancer were included. Adverse events were defined as leptomeningeal disease, radiation necrosis, seizure, and headache. The pooled estimate was calculated using the DerSimonian and Laird approach.
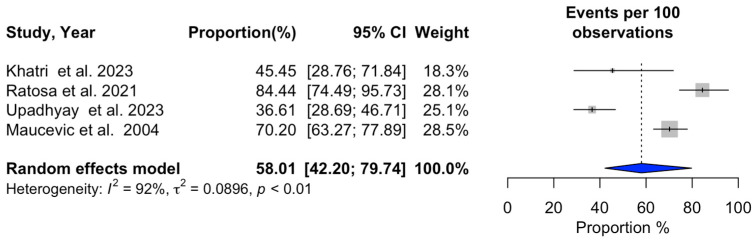
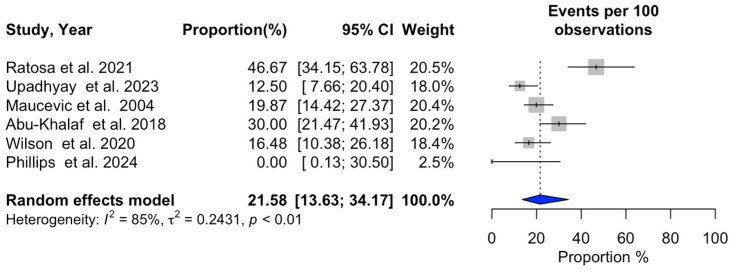
Results: Sixteen studies encompassing 1228 patients met the inclusion criteria. Our analysis revealed a median survival duration of 13.1 ± 3.8 months and a pooled 1-year overall survival rate of 53.1% after SRS treatment. There was a 29% local recurrence rate at 1 year and a 35% overall distant recurrence rate. In addition, our analysis found a relatively low rate of acute adverse events at 15.5%.
Conclusions: SRS demonstrates promising efficacy and safety in managing intracranial metastases from breast cancer, with a favorable toxicity profile.
Keywords: Gamma Knife radiosurgery; breast cancer; intracranial metastasis; stereotactic radiosurgery.
Conflict of interest statement
The author Chirag Shah reports Consultant Impedimed, PreludeDX, and Videra Surgical as conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures






References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
