

Efficacy of Ivermectin, Chloroquine/Hydroxychloroquine, and Azithromycin in Managing COVID-19: A Systematic Review of Phase III Clinical Trials
- PMID: 39457519
- PMCID: PMC11505156
- DOI: 10.3390/biomedicines12102206
Efficacy of Ivermectin, Chloroquine/Hydroxychloroquine, and Azithromycin in Managing COVID-19: A Systematic Review of Phase III Clinical Trials
Abstract
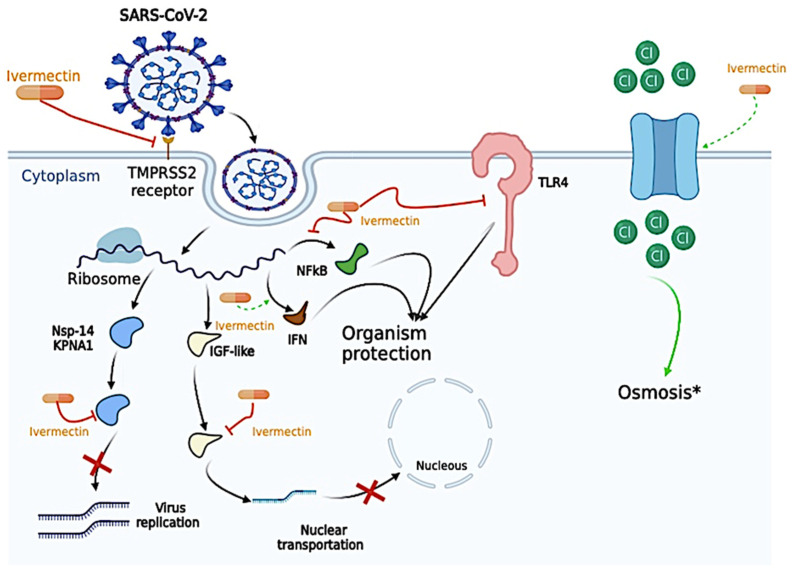
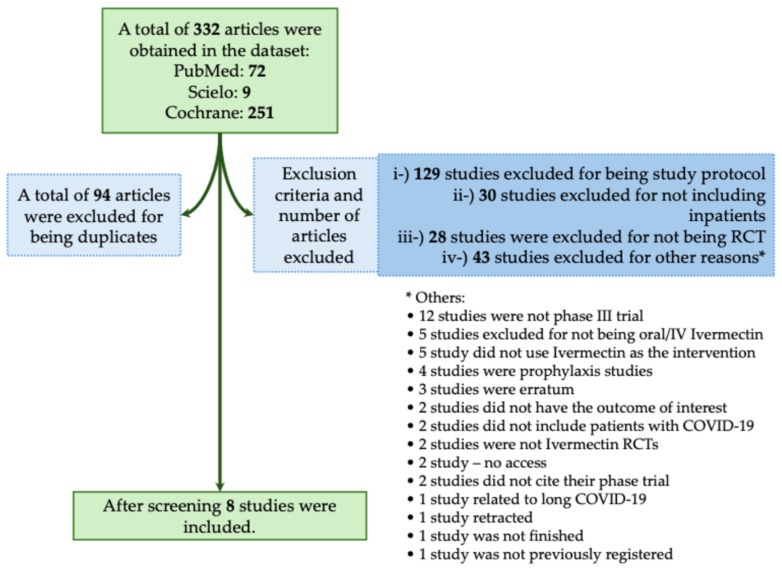
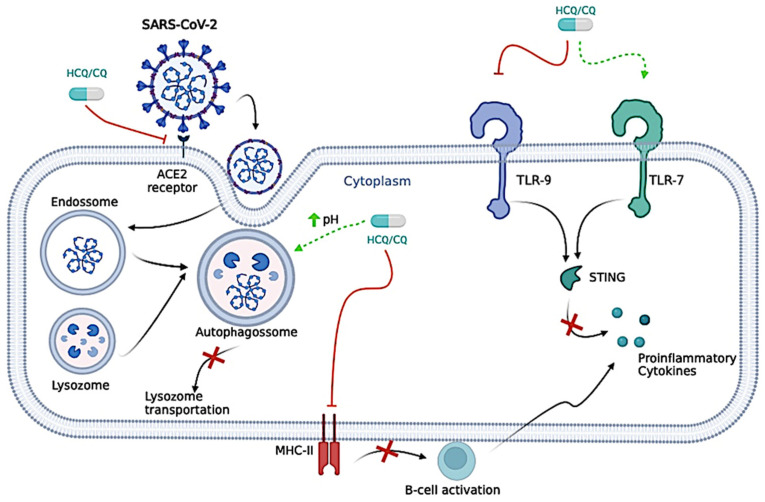
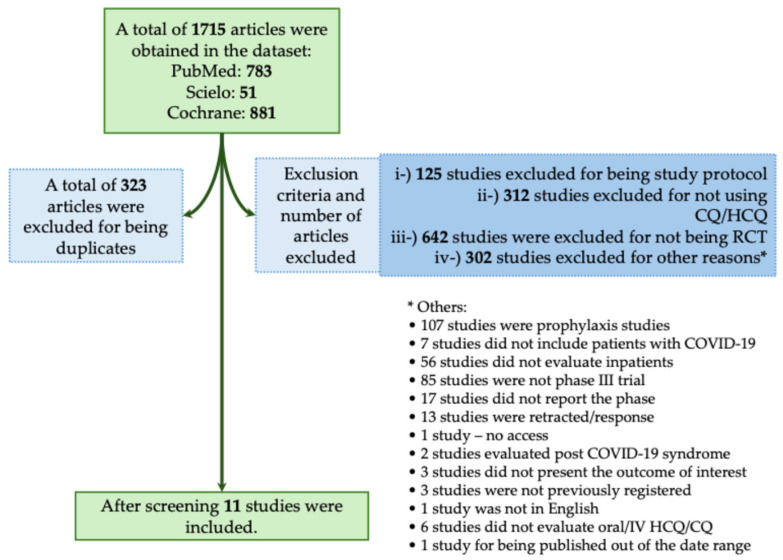
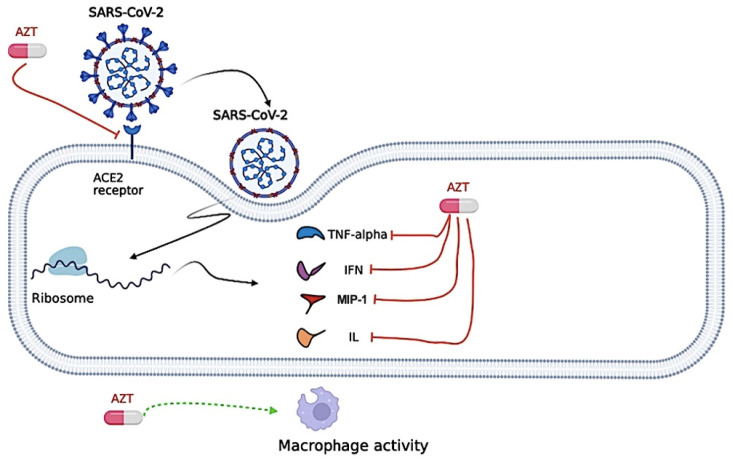
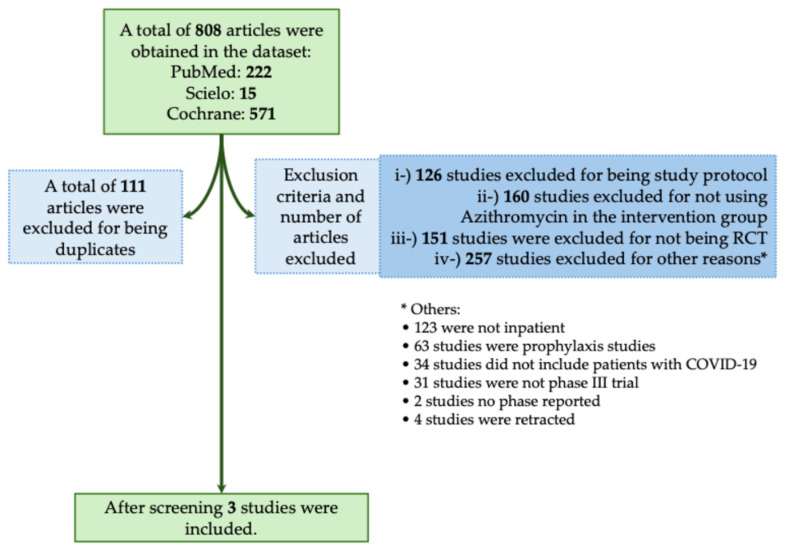
Background: During the coronavirus disease (COVID)-19 pandemic several drugs were used to manage the patients mainly those with a severe phenotype. Potential drugs were used off-label and major concerns arose from their applicability to managing the health crisis highlighting the importance of clinical trials. In this context, we described the mechanisms of the three repurposed drugs [Ivermectin-antiparasitic drug, Chloroquine/Hydroxychloroquine-antimalarial drugs, and Azithromycin-antimicrobial drug]; and, based on this description, the study evaluated the clinical efficacy of those drugs published in clinical trials. The use of these drugs reflects the period of uncertainty that marked the beginning of the COVID-19 pandemic, which made them a possible treatment for COVID-19. Methods: In our review, we evaluated phase III randomized controlled clinical trials (RCTs) that analyzed the efficacy of these drugs published from the COVID-19 pandemic onset to 2023. We included eight RCTs published for Ivermectin, 11 RCTs for Chloroquine/Hydroxychloroquine, and three RCTs for Azithromycin. The research question (PICOT) accounted for P-hospitalized patients with confirmed or suspected COVID-19; I-use of oral or intravenous Ivermectin OR Chloroquine/Hydroxychloroquine OR Azithromycin; C-placebo or no placebo (standard of care); O-mortality OR hospitalization OR viral clearance OR need for mechanical ventilation OR clinical improvement; and T-phase III RCTs. Results: While studying these drugs' respective mechanisms of action, the reasons for which they were thought to be useful became apparent and are as follows: Ivermectin binds to insulin-like growth factor and prevents nuclear transportation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), therefore preventing cell entrance, induces apoptosis, and osmotic cell death and disrupts viral replication. Chloroquine/Hydroxychloroquine blocks the movement of SARS-CoV-2 from early endosomes to lysosomes inside the cell, also, this drug blocks the binding between SARS-CoV-2 and Angiotensin-Converting Enzyme (ACE)-2 inhibiting the interaction between the virus spike proteins and the cell membrane and this drug can also inhibit SARS-CoV-2 viral replication causing, ultimately, the reduction in viral infection as well as the potential to progression for a higher severity phenotype culminating with a higher chance of death. Azithromycin exerts a down-regulating effect on the inflammatory cascade, attenuating the excessive production of cytokines and inducing phagocytic activity, and acts interfering with the viral replication cycle. Ivermectin, when compared to standard care or placebo, did not reduce the disease severity, need for mechanical ventilation, need for intensive care unit, or in-hospital mortality. Only one study demonstrated that Ivermectin may improve viral clearance compared to placebo. Individuals who received Chloroquine/Hydroxychloroquine did not present a lower incidence of death, improved clinical status, or higher chance of respiratory deterioration compared to those who received usual care or placebo. Also, some studies demonstrated that Chloroquine/Hydroxychloroquine resulted in worse outcomes and side-effects included severe ones. Adding Azithromycin to a standard of care did not result in clinical improvement in hospitalized COVID-19 participants. In brief, COVID-19 was one of the deadliest pandemics in modern human history. Due to the potential health catastrophe caused by SARS-CoV-2, a global effort was made to evaluate treatments for COVID-19 to attenuate its impact on the human species. Unfortunately, several countries prematurely justified the emergency use of drugs that showed only in vitro effects against SARS-CoV-2, with a dearth of evidence supporting efficacy in humans. In this context, we reviewed the mechanisms of several drugs proposed to treat COVID-19, including Ivermectin, Chloroquine/Hydroxychloroquine, and Azithromycin, as well as the phase III clinical trials that evaluated the efficacy of these drugs for treating patients with this respiratory disease. Conclusions: As the main finding, although Ivermectin, Chloroquine/Hydroxychloroquine, and Azithromycin might have mechanistic effects against SARS-CoV-2 infection, most phase III clinical trials observed no treatment benefit in patients with COVID-19, underscoring the need for robust phase III clinical trials.
Keywords: antibiotics; azithromycin; chloroquine; clinical trial; coronavirus disease; hydroxychloroquine; ivermectin; severe acute respiratory syndrome coronavirus 2.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
