

Locoregional Therapies for Hepatocellular Carcinoma in Patients with Nonalcoholic Fatty Liver Disease
- PMID: 39457538
- PMCID: PMC11504147
- DOI: 10.3390/biomedicines12102226
Locoregional Therapies for Hepatocellular Carcinoma in Patients with Nonalcoholic Fatty Liver Disease
Abstract
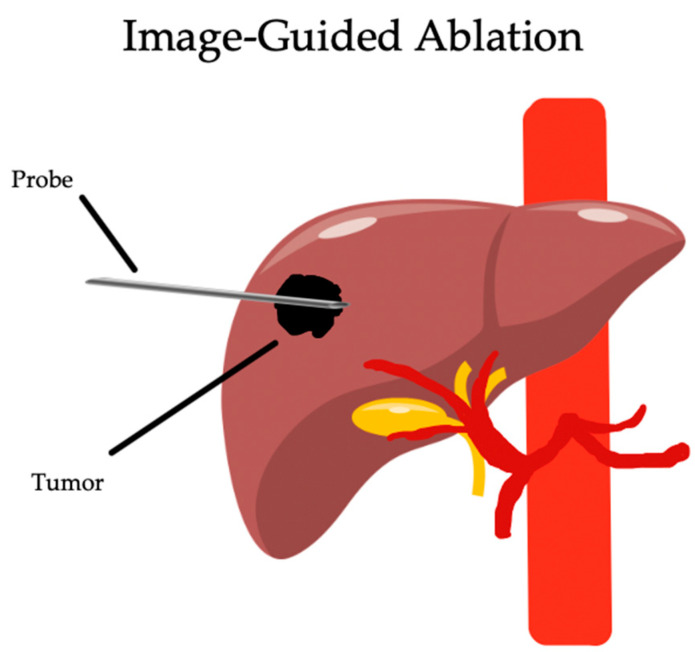
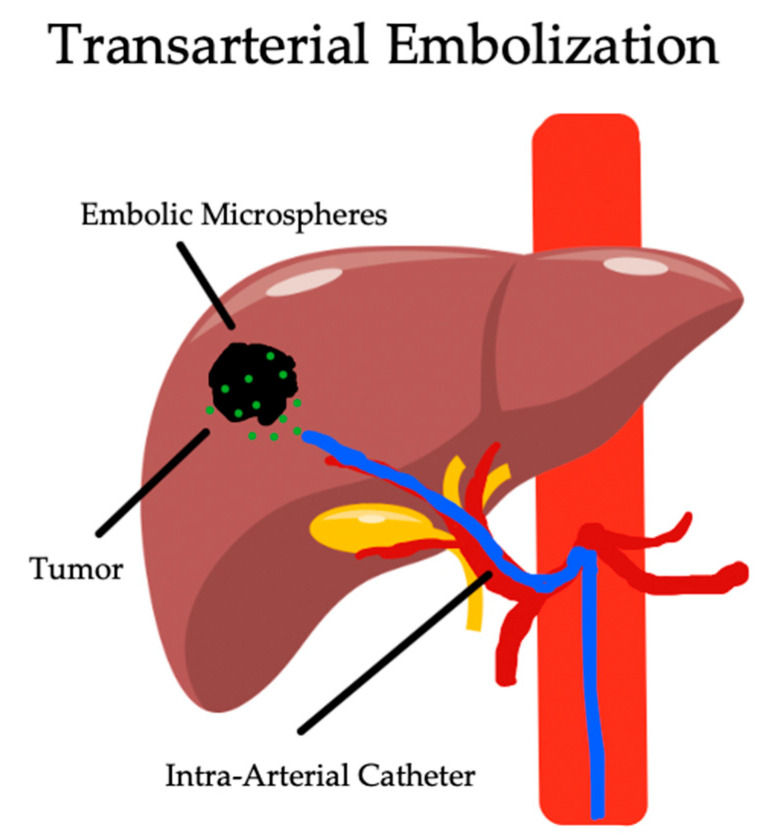
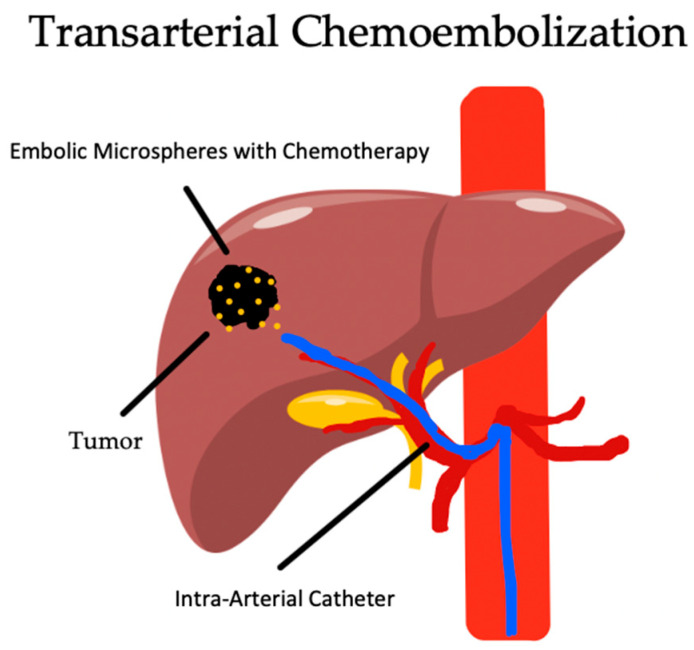
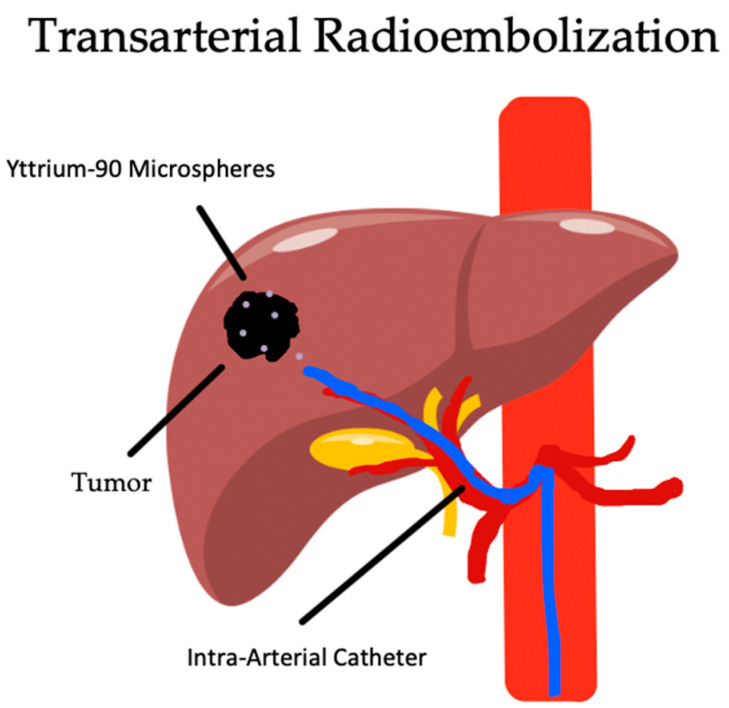
Hepatocellular carcinoma (HCC) is the third most common cause of cancer-related death worldwide with an average five-year survival rate in the US of 19.6%. With the advent of HBV and HCV treatment and prevention, along with the rising rates of obesity, nonalcoholic fatty liver disease (NAFLD) and metabolic syndrome are set to overtake infectious causes as the most common cause of HCC. While surgical resection and transplantation can be curative when amenable, the disease is most commonly unresectable on presentation, and other treatment approaches are the mainstay of therapy. In these patients, locoregional therapies have evolved as a vital tool in both palliation for advanced disease and as a bridge to surgical resection and transplantation. In this review, we will be exploring the primary locoregional therapies for HCC in patients with NAFLD, including transarterial chemoembolization (TACE), bland transarterial embolization (TAE), transarterial radioembolization (TARE), and percutaneous ablation.
Keywords: TACE; TAE; TARE; chemoembolization; hepatocellular carcinoma; metabolic syndrome; nonalcoholic fatty liver disease; nonalcoholic steatohepatitis; radioembolization; transarterial embolization.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
