

Pulsed Field Ablation of Atrial Fibrillation: A Novel Technology for Safer and Faster Ablation
- PMID: 39457545
- PMCID: PMC11504058
- DOI: 10.3390/biomedicines12102232
Pulsed Field Ablation of Atrial Fibrillation: A Novel Technology for Safer and Faster Ablation
Abstract
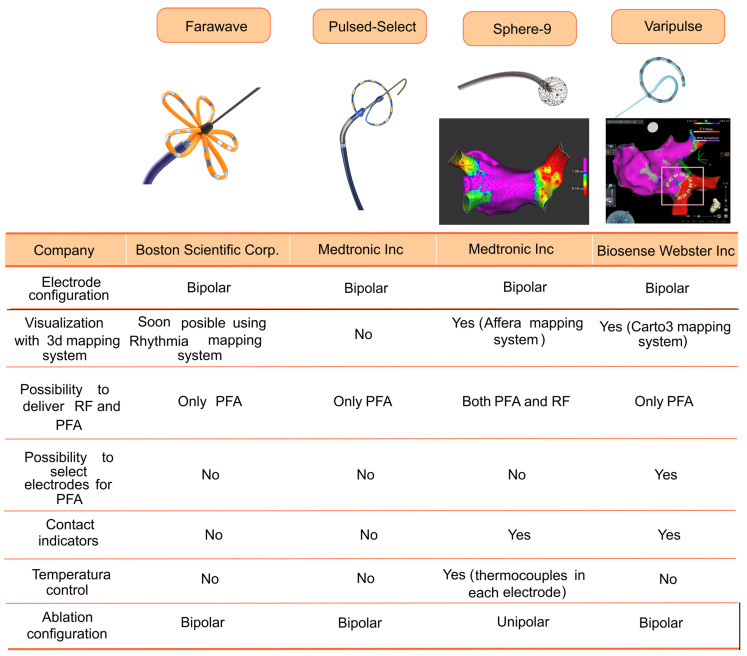
Atrial fibrillation (AF), the most common arrhythmia, is associated with increased morbidity, mortality, and healthcare costs. Evidence indicates that rhythm control offers superior cardiovascular outcomes compared to rate control, especially when initiated early after the diagnosis of AF. Catheter ablation remains the single best therapy for AF; however, it is not free from severe complications and only a small percentage of AF patients in the Western world ultimately receive ablation. Ensuring that AF ablation is safe, effective, and efficient is essential to make it accessible to all patients. With the limitations of traditional thermal ablative energies, pulsed field ablation (PFA) has emerged as a novel non-thermal energy source. PFA targets irreversible electroporation of cardiomyocytes to achieve cell death without damaging adjacent structures. Through its capability to create rapid, selective lesions in myocytes, PFA presents a promising alternative, offering enhanced safety, reduced procedural times, and comparable, if not superior, efficacy to thermal energies. The surge of new evidence makes it challenging to stay updated and understand the possibilities and challenges of PFA. This review aims to summarize the most significant advantages of PFA and how this has translated to the clinical arena, where four different catheters have received CE-market approval for AF ablation. Further research is needed to explore whether adding new ablation targets, previously avoided due to risks associated with thermal energies, to pulmonary vein isolation can improve the efficacy of AF ablation. It also remains to see whether a class effect exists or if different PFA technologies can yield distinct clinical outcomes given that the optimization of PFA parameters has largely been empirical.
Keywords: atrial fibrillation; catheter ablation; electroporation; pulsed field ablation.
Conflict of interest statement
Pablo Ávila, Felipe Atienza and Ángel Arenal have received consultancy fees from Medtronic Inc. Pablo Ávila and Ángel Arenal have received consultancy fees from Boston Scientific Corp. Ángel Arenal, Alejandro Carta and Esteban González-Torrecilla participated as investigator and sub-investigators, respectively, in the PULSED-AF pivotal trial. The other authors have no conflicts of interest to declare.
Figures





References
-
- Tzeis S., Gerstenfeld E.P., Kalman J., Saad E.B., Shamloo A.S., Andrade J.G., Barbhaiya C.R., Baykaner T., Boveda S., Calkins H., et al. 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation. Europace. 2024;26:5–8. doi: 10.1093/europace/euae043. - DOI
-
- Camm A.J., Naccarelli G.V., Mittal S., Crijns H.J.G.M., Hohnloser S.H., Ma C.S., Natale A., Turakhia M.P., Kirchhof P. The Increasing Role of Rhythm Control in Patients with Atrial Fibrillation: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022;79:1932–1948. doi: 10.1016/j.jacc.2022.03.337. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
