

Bedside Neuromodulation of Persistent Pain and Allodynia with Caloric Vestibular Stimulation
- PMID: 39457677
- PMCID: PMC11505407
- DOI: 10.3390/biomedicines12102365
Bedside Neuromodulation of Persistent Pain and Allodynia with Caloric Vestibular Stimulation
Abstract
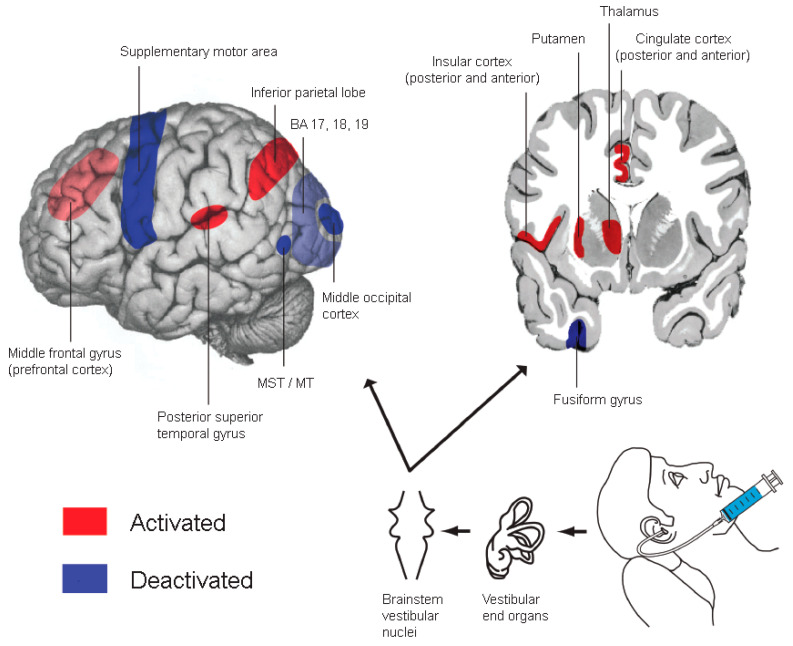
Background: Caloric vestibular stimulation (CVS) is a well-established neurological diagnostic technique that also induces many phenomenological modulations, including reductions in phantom limb pain (PLP), spinal cord injury pain (SCIP), and central post-stroke pain.
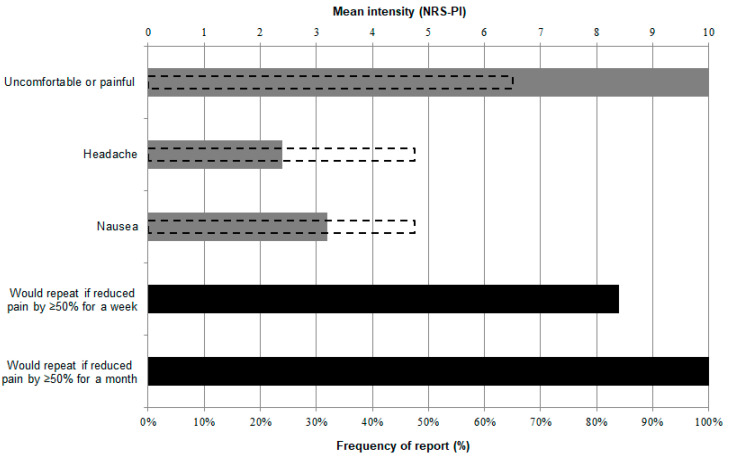
Objective: We aimed to assess in a variety of persistent pain (PP) conditions (i) short-term pain modulation by CVS relative to a forehead ice pack cold-arousal control procedure and (ii) the duration and repeatability of CVS modulations. The tolerability of CVS was also assessed and has been reported separately.
Methods: We conducted a convenience-based non-randomised single-blinded placebo-controlled study. Thirty-eight PP patients were assessed (PLP, n = 8; SCIP, n = 12; complex regional pain syndrome, CRPS, n = 14; non-specific PP, n = 4). Patients underwent 1-3 separate-day sessions of iced-water right-ear CVS. All but four also underwent the ice pack procedure. Analyses used patient-reported numerical rating scale pain intensity (NRS-PI) scores for pain and allodynia.
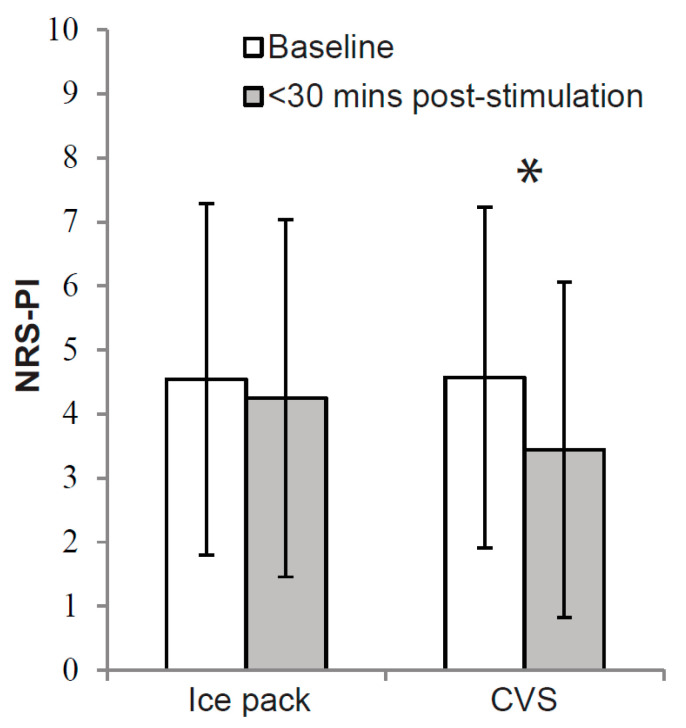
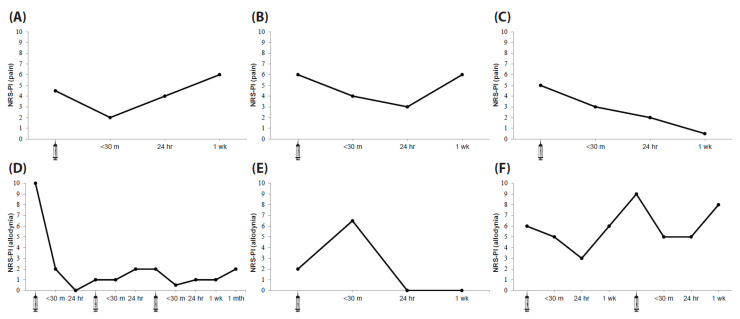
Results: Across all groups, NRS-PI for pain was significantly lower within 30 min post-CVS than post-ice pack (p < 0.01). Average reductions were 24.8% (CVS) and 6.4% (ice pack). CRPS appeared most responsive to CVS, while PLP and SCIP responses were less than expected from previous reports. The strongest CVS pain reductions lasted hours to over three weeks. CVS also induced substantial reductions in allodynia in three of nine allodynic CRPS patients, lasting 24 h to 1 month. As reported elsewhere, only one patient experienced emesis and CVS was widely rated by patients as a tolerable PP management intervention.
Conclusions: Although these results require interpretative caution, CVS was found to modulate pain relative to an ice pack control. CVS also modulated allodynia in some cases. CVS should be examined for pain management efficacy using randomised controlled trials.
Keywords: allodynia; caloric vestibular stimulation; complex regional pain syndrome; non-invasive brain stimulation; persistent pain; phantom limb pain; spinal cord injury pain; vestibular neuromodulation.
Conflict of interest statement
S.M.M. has received equipment for research from Soterix Medical Inc. P.B.F. has received equipment for research from MagVenture A/S, Medtronic Ltd., Neuronetics and Brainsway Ltd. and funding for research from Neuronetics. He is on scientific advisory boards for Bionomics Ltd. and LivaNova and is a founder of TMS Clinics Australia. S.M.M. and A.K.N. have received funding from Monash Institute of Medical Engineering to examine methods for CVS self-administration. If such methods are commercialised, Monash University, Monash Alfred Psychiatry Research Centre and authors S.M.M. and A.K.N. would receive royalties. The remaining authors have no competing interest related to this work to disclose.
Figures
Similar articles
-
Post-stroke tactile allodynia and its modulation by vestibular stimulation: a MEG case study.Acta Neurol Scand. 2009 Jun;119(6):404-9. doi: 10.1111/j.1600-0404.2008.01106.x. Epub 2008 Oct 6. Acta Neurol Scand. 2009. PMID: 18853944
-
Allodynia, Hyperalgesia, (Quantitative) Sensory Testing and Conditioned Pain Modulation in Patients With Complex Regional Pain Syndrome Before and After Spinal Cord Stimulation Therapy.Neuromodulation. 2023 Jan;26(1):78-86. doi: 10.1016/j.neurom.2022.06.009. Epub 2022 Aug 30. Neuromodulation. 2023. PMID: 36050204 Clinical Trial.
-
Beneficial effects of caloric vestibular stimulation on denial of illness and manic delusions in schizoaffective disorder: a case report.Brain Stimul. 2012 Jul;5(3):267-273. doi: 10.1016/j.brs.2011.03.004. Epub 2011 Apr 8. Brain Stimul. 2012. PMID: 21783454
-
A Review of Neuromodulation for Treatment of Complex Regional Pain Syndrome in Pediatric Patients and Novel Use of Dorsal Root Ganglion Stimulation in an Adolescent Patient With 30-Month Follow-Up.Neuromodulation. 2021 Jun;24(4):634-638. doi: 10.1111/ner.13257. Epub 2020 Aug 28. Neuromodulation. 2021. PMID: 32856364 Review.
-
The use of tDCS and CVS as methods of non-invasive brain stimulation.Brain Res Rev. 2007 Dec;56(2):346-61. doi: 10.1016/j.brainresrev.2007.08.001. Epub 2007 Aug 28. Brain Res Rev. 2007. PMID: 17900703 Review.
Cited by
-
A review of synergistic strategies in cancer therapy: resveratrol-loaded hydrogels for targeted and multimodal treatment.Discov Oncol. 2025 Jul 21;16(1):1382. doi: 10.1007/s12672-025-03079-w. Discov Oncol. 2025. PMID: 40690143 Free PMC article. Review.
-
Vestibular Versus Cochlear Stimulation on the Relief of Phantom Pain After Traumatic Finger Amputation.Biomedicines. 2025 Jun 30;13(7):1601. doi: 10.3390/biomedicines13071601. Biomedicines. 2025. PMID: 40722675 Free PMC article.
References
-
- Andersson G.B.J., Watkins-Castillo S.I. The Burden of Musculoskeletal Diseases in the United States. 3rd ed. United States Bone and Joint Initiative; Rosemont, IL, USA: 2014.
-
- Deloitte Access Economics . The Cost of Pain in Australia. Painaustralia; Deakin, Australia: 2019.
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
