

Elevated Cardiac Troponin Levels as a Predictor of Increased Mortality Risk in Non-Cardiac Critically Ill Patients Admitted to a Medical Intensive Care Unit
- PMID: 39457975
- PMCID: PMC11508240
- DOI: 10.3390/jcm13206025
Elevated Cardiac Troponin Levels as a Predictor of Increased Mortality Risk in Non-Cardiac Critically Ill Patients Admitted to a Medical Intensive Care Unit
Abstract
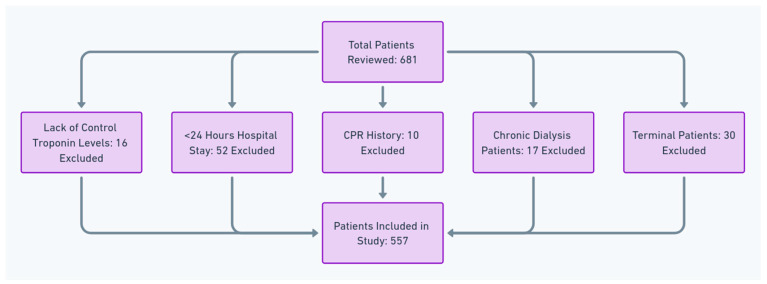
Background: Cardiac troponin I (TnI) is a specific marker of myocardial damage used in the diagnosis of acute coronary syndrome (ACS). TnI levels can also be elevated in patients without ACS, which is linked to a worse prognosis and mortality. We evaluated the clinical implications and prognostic significance of serum TnI levels in critically ill non-cardiac patients admitted to the intensive care unit (ICU) at a tertiary-level hospital. Materials and Methods: A three-year retrospective study including the years 2017-2020 was conducted to evaluate in-hospital mortality during ICU stay and mortality rates at 28 and 90 days, as well as one and two years after admission, in 557 patients admitted to the medical ICU for non-cardiac causes. Results: TnI levels were elevated in 206 (36.9%) patients. Patients with elevated TnI levels were significantly older and had higher rates of comorbidities, including chronic heart failure, coronary heart disease, and chronic kidney disease (p < 0.05 for all). Patients with elevated TnI levels required more invasive mechanical ventilation, vasopressor infusion, and dialysis in the ICU and experienced more shock within the first 72 h (p = 0.001 for all). High TnI levels were associated with higher Acute Physiological and Chronic Health Evaluation (APACHE) II (27.6 vs. 20.3, p = 0.001) and Sequential Organ Failure assessment (8.8 vs. 5.26, p = 0.001) scores. Elevated TnI levels were associated with higher mortality rates at 28 days (58.3% vs. 19.4%), 90 days (69.9% vs. 35.0%), one year (78.6% vs. 46.2%), and two years (82.5% vs. 55.6%) (p < 0.001 for all). Univariate logistic regression analysis revealed that high TnI levels were a strong independent predictor of mortality at all time points: 28 days (OR = 1.2, 95% CI: 1.108-1.3, p < 0.001), 90 days (OR = 1.207, 95% CI: 1.095-1.33, p = 0.001), one year (OR = 1.164, 95% CI: 1.059-1.28, p = 0.002), and two year (OR = 1.119, 95% CI: 1.026-1.22, p = 0.011). Multivariate analysis revealed that age, albumin level, APACHE II score, and requirements for dialysis and vasopressor use in the ICU were important predictors of mortality across all timeframes, but elevated TnI levels were not. Conclusions: Elevated TnI levels in critically ill non-cardiac patients are markers of disease severity. While elevated TnI levels were significant predictors of mortality in the univariate analysis, they lost significance in the multivariate model when adjusted for other factors. Patients with elevated TnI levels had higher mortality rates across all timeframes, from 28 days to two years.
Keywords: APACHE II scores; SOFA scores; Troponin I (TnI); long-term mortality; medical intensive care unit (MICU); short-term mortality.
Conflict of interest statement
The author declares no conflict of interest.
Figures
Similar articles
-
Use of admission troponin in critically ill medical patients.J Intensive Care Med. 2005 Nov-Dec;20(6):334-8. doi: 10.1177/0885066605280322. J Intensive Care Med. 2005. PMID: 16280406
-
[Clinical predictive value of short-term dynamic changes in platelet counts for prognosis of sepsis patients in intensive care unit: a retrospective cohort study in adults].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Mar;32(3):301-306. doi: 10.3760/cma.j.cn121430-20190909-00069. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32385993 Chinese.
-
Early troponin I in critical illness and its association with hospital mortality: a cohort study.Crit Care. 2017 Aug 16;21(1):216. doi: 10.1186/s13054-017-1800-4. Crit Care. 2017. PMID: 28814347 Free PMC article.
-
Cardiac injury associated with severe disease or ICU admission and death in hospitalized patients with COVID-19: a meta-analysis and systematic review.Crit Care. 2020 Jul 28;24(1):468. doi: 10.1186/s13054-020-03183-z. Crit Care. 2020. PMID: 32723362 Free PMC article.
-
Cardiooncology in the ICU - Cardiac Urgencies in Cancer Care.J Intensive Care Med. 2024 Dec 5:8850666241303461. doi: 10.1177/08850666241303461. Online ahead of print. J Intensive Care Med. 2024. PMID: 39632745 Review.
Cited by
-
Predicting the risk of heart failure after acute myocardial infarction using an interpretable machine learning model.Front Cardiovasc Med. 2025 Jan 24;12:1444323. doi: 10.3389/fcvm.2025.1444323. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 39925976 Free PMC article.
References
-
- Wu T.T., Yuan A., Chen C.Y., Chen W.J., Luh K.T., Kuo S.H., Lin F.Y., Yang P.C. Cardiac troponin I levels are a risk factor for mortality and multiple organ failure in non-cardiac critically ill patients and have an additive effect to the APACHE II score in outcome prediction. Shock. 2004;22:95–101. doi: 10.1097/01.shk.0000132484.97424.32. - DOI - PubMed
-
- Babuin L., Vasile V.C., Perez J.A.R., Alegria J.R., Chai H.-S., Afessa B., Jaffe A.S. Elevated cardiac troponin is an independent risk factor for short- and long-term mortality in medical intensive care unit patients. Crit. Care Med. 2008;36:759–765. doi: 10.1097/CCM.0B013E318164E2E4. - DOI - PubMed
-
- Botto F., Alonso-Coello P., Chan M., Vascular events In non-cardiac Surgery patIents cOhort evaluatioN (VISION) Writing Group, on behalf of The Vascular events In non-cardiac Surgery patIents cOhort evaluatioN (VISION) Investigators. Appendix 1. The Vascular events In non-cardiac Surgery patIents cOhort evaluatioN (VISION) Study Investigators Writing Group. Appendix 2. The Vascular events In non-cardiac Surgery patIents cOhort evaluatioN Operations Committee. Vascular events In non-cardiac Surgery patIents cOhort evaluatioN VISION Study Investigators Myocardial injury after non-cardiac surgery: A large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120:564–578. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
