

Cardiometabolic Morbidity (Obesity and Hypertension) in PTSD: A Preliminary Investigation of the Validity of Two Structures of the Impact of Event Scale-Revised
- PMID: 39457995
- PMCID: PMC11509123
- DOI: 10.3390/jcm13206045
Cardiometabolic Morbidity (Obesity and Hypertension) in PTSD: A Preliminary Investigation of the Validity of Two Structures of the Impact of Event Scale-Revised
Abstract
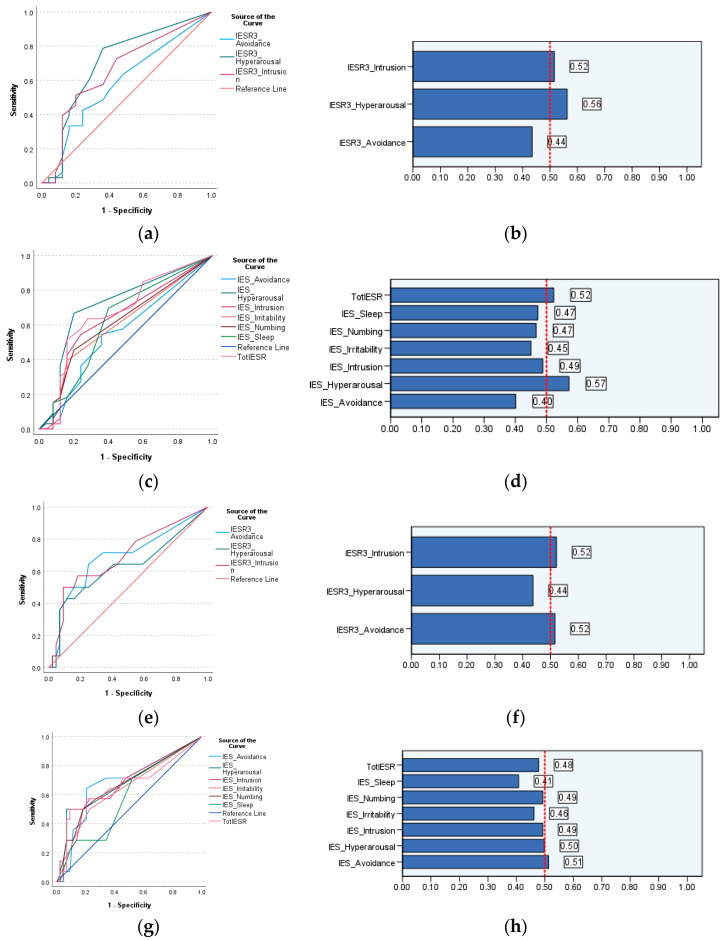
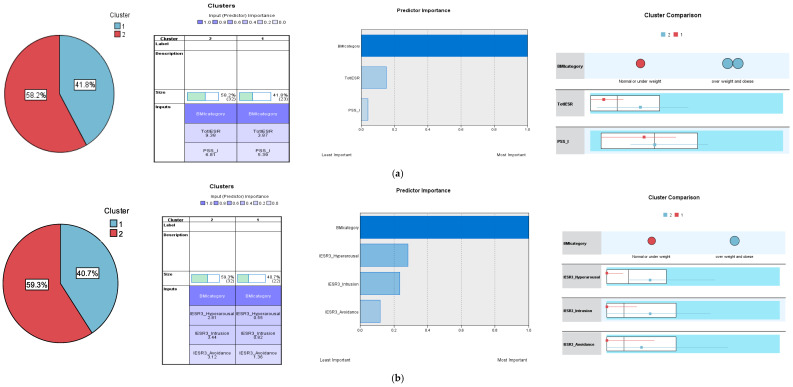
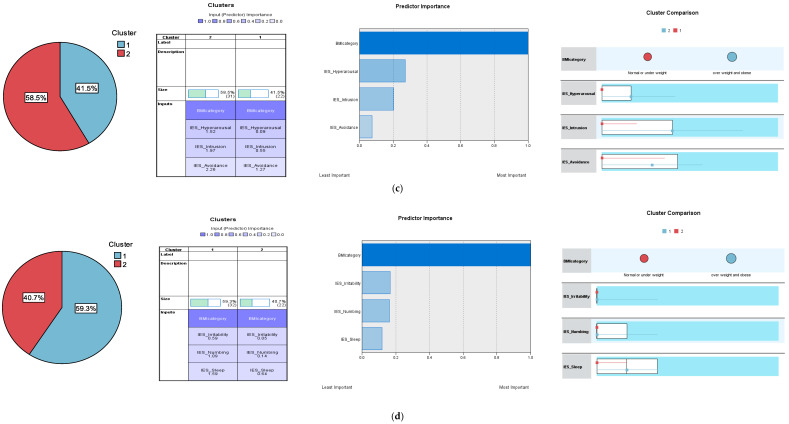
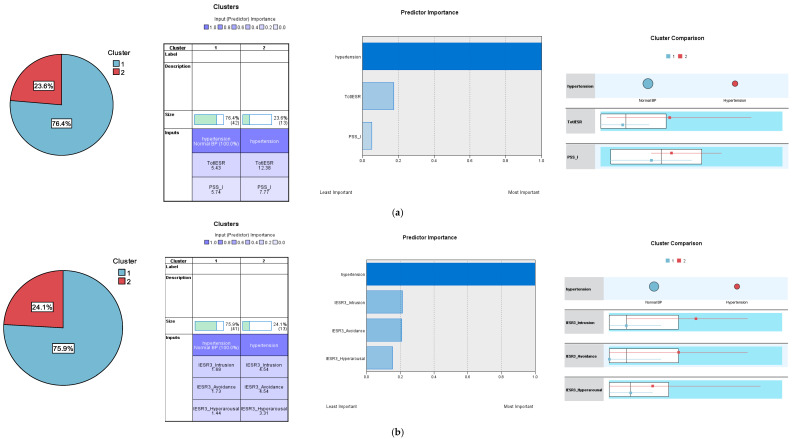
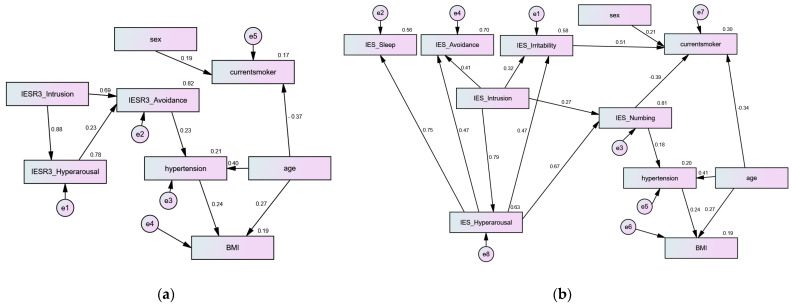
Background: Posttraumatic stress disorder (PTSD) and/or specific PTSD symptoms may evoke maladaptive behaviors (e.g., compulsive buying, disordered eating, and an unhealthy lifestyle), resulting in adverse cardiometabolic events (e.g., hypertension and obesity), which may implicate the treatment of this complex condition. The diagnostic criteria for PTSD have lately expanded beyond the three common symptoms (intrusion, avoidance, and hyperarousal). Including additional symptoms such as emotional numbing, sleep disturbance, and irritability strengthens the representation of the Impact of Event Scale-Revised (IES-R), suggesting that models with four, five, or six dimensions better capture its structure compared to the original three-dimensional model. Methods: Using a convenience sample of 58 Russian dental healthcare workers (HCWs: mean age = 44.1 ± 12.2 years, 82.8% females), this instrumental study examined the convergent, concurrent, and criterion validity of two IES-R structures: IES-R3 and IES-R6. Results: Exploratory factor analysis uncovered five factors, which explained 76.0% of the variance in the IES-R. Subscales of the IES-R3 and the IES-R6 expressed good internal consistency (coefficient alpha range = 0.69-0.88), high convergent validity (item total correlations r range = 0.39-0.81, and correlations with the IES-R's total score r range = 0.62-0.92), excellent concurrent validity through strong correlations with the PTSD Symptom Scale-Self Report (PSS-SR: r range = 0.42-0.69), while their criterion validity was indicated by moderate-to-low correlations with high body mass index (BMI: r range = 0.12-0.39) and the diagnosis of hypertension (r range = 0.12-0.30). In the receiver-operating characteristic (ROC) curve analysis, all IES-R models were perfectly associated with the PSS-SR (all areas under the curve (AUCs) > 0.9, p values < 0.001). The IES-R, both hyperarousal subscales, and the IES-R3 intrusion subscale were significantly associated with high BMI. Both avoidance subscales and the IES-R3 intrusion subscale, not the IES-R, were significantly associated with hypertension. In the two-step cluster analysis, five sets of all trauma variables (IES-R3/IES-R6, PSS-SR) classified the participants into two clusters according to their BMI (normal weight/low BMI vs. overweight/obese). Meanwhile, only the IES-R, PSS-SR, and IES-R3 dimensions successfully classified participants as having either normal blood pressure or hypertension. Participants in the overweight/obese and hypertensive clusters displayed considerably higher levels of most trauma symptoms. Input variables with the highest predictor importance in the cluster analysis were those variables expressing significant associations in correlations and ROC analyses. However, neither IES-R3 nor IES-R6 contributed to BMI or hypertension either directly or indirectly in the path analysis. Meanwhile, age significantly predicted both health conditions and current smoking. Irritability and numbing were the only IES-R dimensions that significantly contributed to current smoking. Conclusions: The findings emphasize the need for assessing the way through which various PTSD symptoms may implicate cardiometabolic dysfunctions and their risk factors (e.g., smoking and the intake of unhealthy foods) as well as the application of targeted dietary and exercise interventions to lower physical morbidity in PTSD patients. However, the internal and external validity of our tests may be questionable due to the low power of our sample size. Replicating the study in larger samples, which comprise different physical and mental conditions from heterogenous cultural contexts, is pivotal to validate the results (e.g., in specific groups, such as those with confirmed traumatic exposure and comorbid mood dysfunction).
Keywords: cardiovascular disorders/CVDs/cardiometabolic*/hypertension; cutoff score/cutoff point; dental healthcare workers; diet*/high-sugar/high fat; impact of event scale-revised/IES-R/posttraumatic stress disorder/PTSD; obesity/high body mass index/metabolic dysfunction; receiver operator curve (ROC); sleep disturbance/irritability/emotional numbing; smoking/behavioral risk factors; three factors/six factors/dimensions.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR. American Psychiatric Association; Washington, DC, USA: 2022.
-
- Butler O., Willmund G., Gleich T., Zimmermann P., Lindenberger U., Gallinat J., Kühn S. Cognitive Reappraisal and Expressive Suppression of Negative Emotion in Combat-Related Posttraumatic Stress Disorder: A Functional MRI Study. Cogn. Ther. Res. 2019;43:236–246. doi: 10.1007/s10608-018-9905-x. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
