

Advanced Lung Cancer Inflammation Index as Predictor of All-Cause Mortality in ST-Elevation Myocardial Infarction Patients Undergoing Primary Percutaneous Coronary Intervention
- PMID: 39458009
- PMCID: PMC11508711
- DOI: 10.3390/jcm13206059
Advanced Lung Cancer Inflammation Index as Predictor of All-Cause Mortality in ST-Elevation Myocardial Infarction Patients Undergoing Primary Percutaneous Coronary Intervention
Abstract
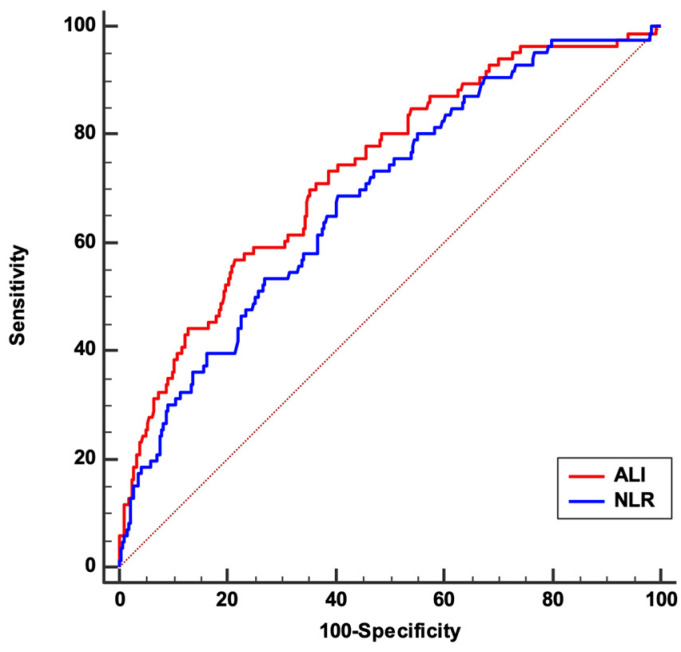
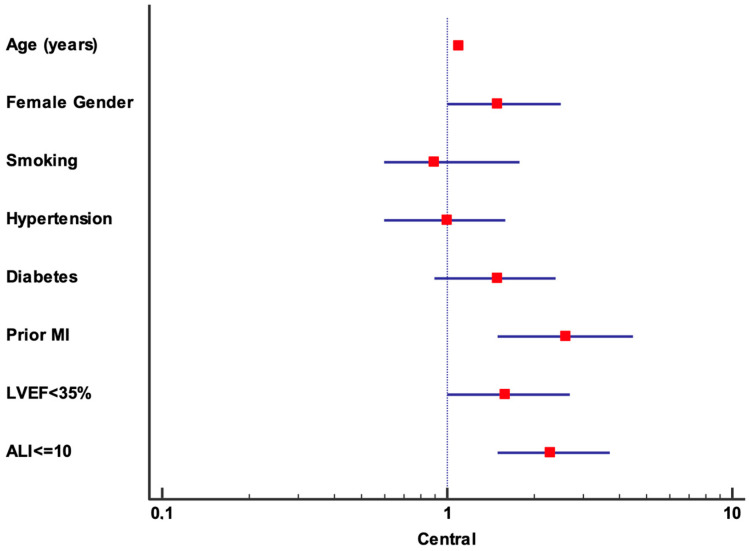
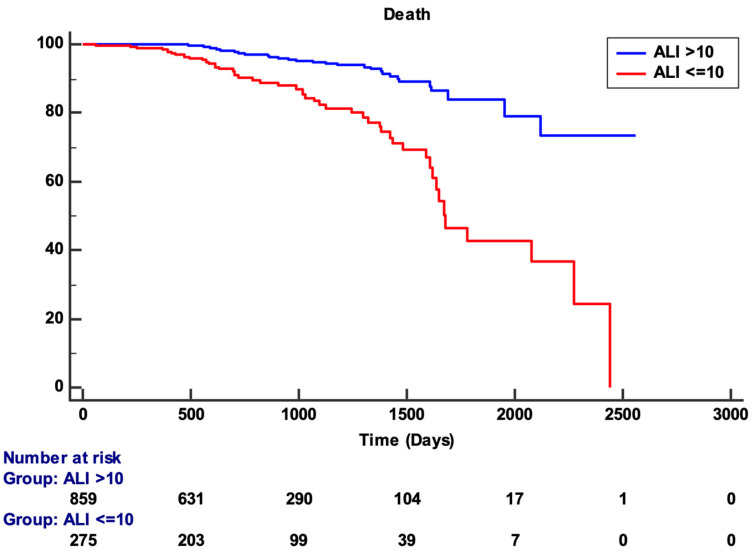
Background: The advanced lung cancer inflammation index (ALI) is an independent prognostic biomarker used to assess inflammation and nutritional status in various cancers, heart failure, and acute coronary syndromes. This study investigates the prognostic significance of ALI in patients experiencing ST-elevation myocardial infarction (STEMI) treated with primary percutaneous coronary intervention (pPCI), comparing its predictive abilities with the established Neutrophil-Lymphocyte Ratio (NLR). Methods: We conducted a retrospective analysis of 1171 patients from the Matrix Registry, encompassing demographic and clinical data for STEMI cases treated with pPCI, and ALI was determined using the formula [serum albumin (g/dL) × body mass index (kg/m2)]/NLR at the time of hospital admission. The primary outcome was all-cause mortality. Results: Of the 1171 patients, 86 died during the follow-up period. Univariate analysis identified age, female gender, smoking, hypertension, diabetes, prior myocardial infarction (PMI), lower left ventricular ejection fraction (LVEF), and reduced ALI as factors associated with mortality. Multivariate analysis confirmed age (HR: 1.1, 95% CI: 1.05-1.11, p < 0.001) and PMI (HR: 2.4, 95% CI: 1.4-4.3, p = 0.001) as prominent independent predictors, alongside ALI (HR: 0.95, 95% CI: 0.92-0.97, p < 0.001) and LVEF (HR: 0.98, 95% CI: 0.97-0.99, p = 0.04). An ALI cut-off of ≤10 indicated a higher mortality risk (HR: 2.3, 95% CI: 1.5-3.7, p < 0.001). The area under the curve for ALI (0.732) surpassed that for NLR (0.685), demonstrating ALI's superior predictive capability. Conclusions: ALI is an independent prognostic factor for all-cause mortality in STEMI patients undergoing pPCI, showing greater discriminatory power than NLR, particularly in patients with ALI values ≤ 10, who face a 2.3-fold higher mortality risk.
Keywords: ST-elevation myocardial infarction; inflammation; malnutrition; mortality; neutrophil-to-lymphocyte ratio; primary PCI; vanced lung cancer inflammation index.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Elendu C., Amaechi D.C., Elendu T.C., Omeludike E.K., Alakwe-Ojimba C.E., Obidigbo B., Akpovona O.L., Oros Sucari Y.P., Saggi S.K., Dang K., et al. Comprehensive Review of ST-Segment Elevation Myocardial Infarction: Understanding Pathophysiology, Diagnostic Strategies, and Current Treatment Approaches. Medicine. 2023;102:e35687. doi: 10.1097/MD.0000000000035687. - DOI - PMC - PubMed
-
- Yamashita Y., Shiomi H., Morimoto T., Yaku H., Furukawa Y., Nakagawa Y., Ando K., Kadota K., Abe M., Nagao K., et al. Cardiac and Noncardiac Causes of Long-Term Mortality in ST-Segment-Elevation Acute Myocardial Infarction Patients Who Underwent Primary Percutaneous Coronary Intervention. Circ. Cardiovasc. Qual. Outcomes. 2017;10:e002790. doi: 10.1161/CIRCOUTCOMES.116.002790. - DOI - PubMed
-
- Garcia-Osuna A., Sans-Rosello J., Ferrero-Gregori A., Alquezar-Arbe A., Sionis A., Ordóñez-Llanos J. Risk Assessment after ST-Segment Elevation Myocardial Infarction: Can Biomarkers Improve the Performance of Clinical Variables? J. Clin. Med. 2022;11:1266. doi: 10.3390/jcm11051266. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
