

Optimization of Exocrine Pancreatic Insufficiency in Pancreatic Adenocarcinoma Patients
- PMID: 39458494
- PMCID: PMC11510683
- DOI: 10.3390/nu16203499
Optimization of Exocrine Pancreatic Insufficiency in Pancreatic Adenocarcinoma Patients
Abstract
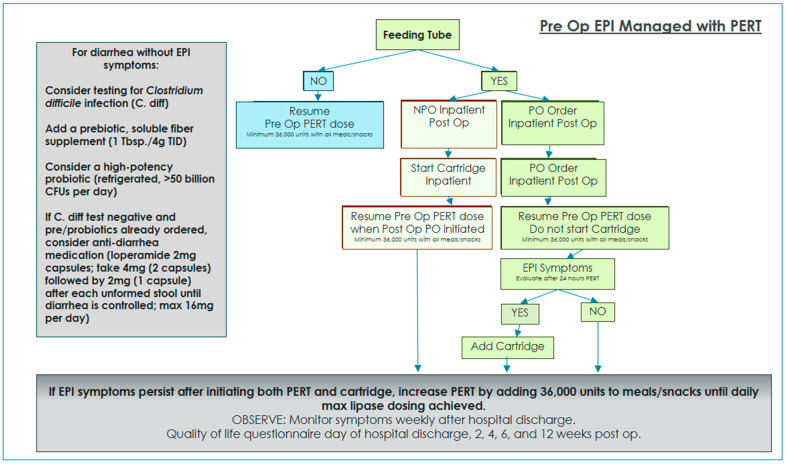
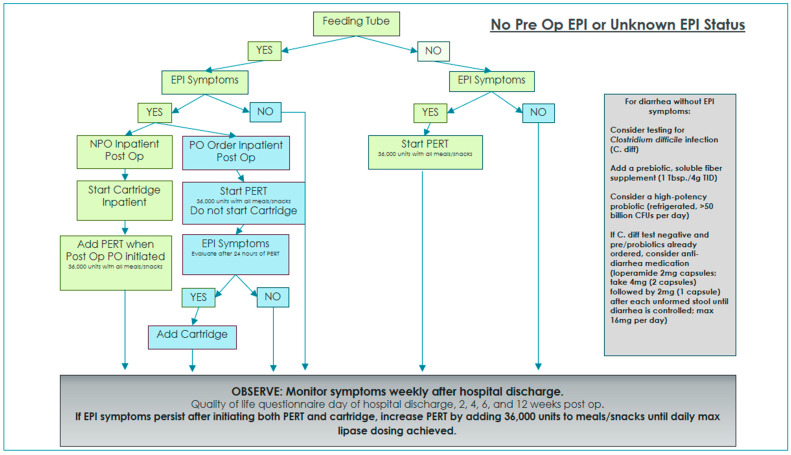
Background/objectives: This study explores the optimization of exocrine pancreatic insufficiency (EPI) management in pancreatic adenocarcinoma patients, focusing on the scientific advancements and technological interventions available to improve patient outcomes, including oral pancreatic enzyme replacement therapy (PERT) and immobilized lipase cartridge (RELiZORB®). This was a prospective Institutional Review Board (IRB)-approved study from October 2019 through to August 2021 at the Louisville Medical Center in collaboration with Norton Healthcare and the University of Louisville Division of Surgical Oncology. Patients with a diagnosis of pancreatic adenocarcinoma (Stage 2 or 3) who underwent oncologic surgical resection were included in this study.
Methods: Patients were contacted at pre-defined intervals (prior to surgery, before hospital discharge, and 2, 4, 6, and 12 weeks after surgery) to complete nutrition evaluation, EPI assessment, and quality of life questionnaires to identify the severity and frequency of gastrointestinal (GI) symptoms.
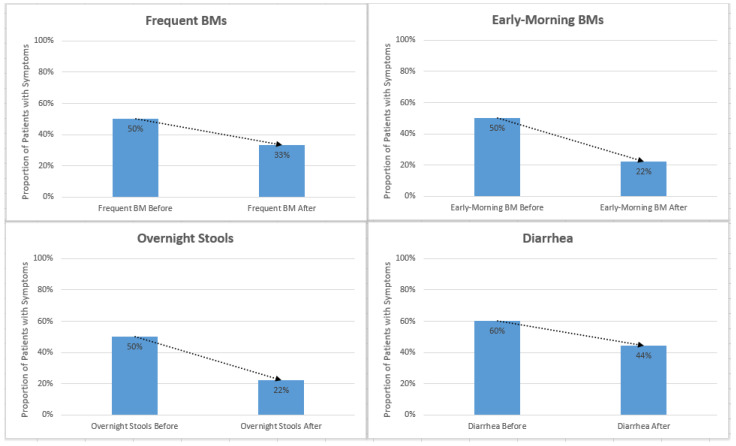
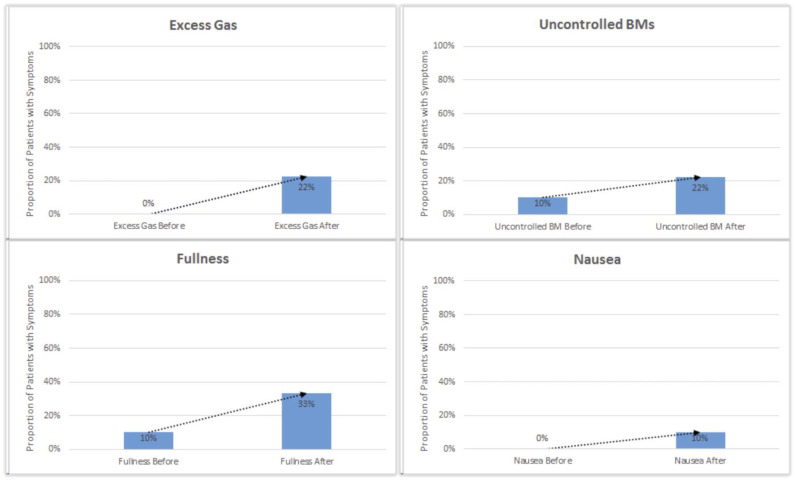
Results: EPI symptoms were reported in 28 of the 35 total patients studied (80%). Jejunostomy tubes were placed during oncologic surgery in 25 of the 35 total patients studied (71%), and 12 of the 25 patients with a jejunostomy tube utilized enzyme cartridges to manage EPI symptoms while on supplemental tube feeding (48%). EPI symptoms were reported in 8 of the 10 patients without a feeding tube (80%), and their EPI symptoms were managed with PERT alone. EPI interventions, both oral PERT and immobilized cartridges, were associated with a decrease in EPI symptoms after surgery and improved quality of life (QOL).
Conclusions: Overall, early optimization of EPI is crucial to enhance overall patient care, return to oncology therapy after surgery, and improve quality of life in pancreatic adenocarcinoma patients.
Keywords: exocrine pancreatic insufficiency; malabsorption; pancreatectomy.
Conflict of interest statement
Charles R. Scoggins, Prejesh Philips, Michael E. Egger, and Robert C.G. Martin II have no conflicts of interest or financial ties to disclose. Jaclyn Moore participates on the speaker’s bureau for Alcresta Therapeutics and AbbVie Inc.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
