

Fast Clinical Response of Bimekizumab in Nail Psoriasis: A Retrospective Multicenter 36-Week Real-Life Study
- PMID: 39459016
- PMCID: PMC11510175
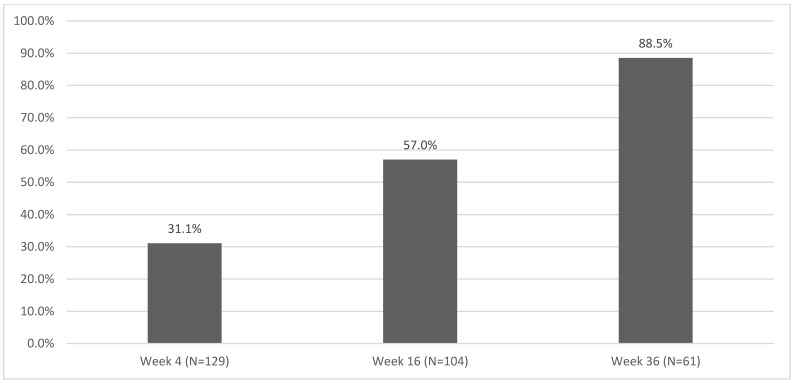
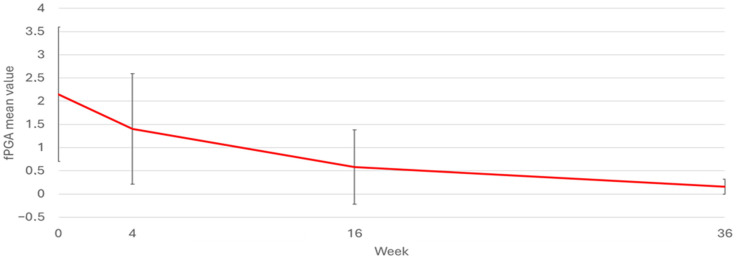
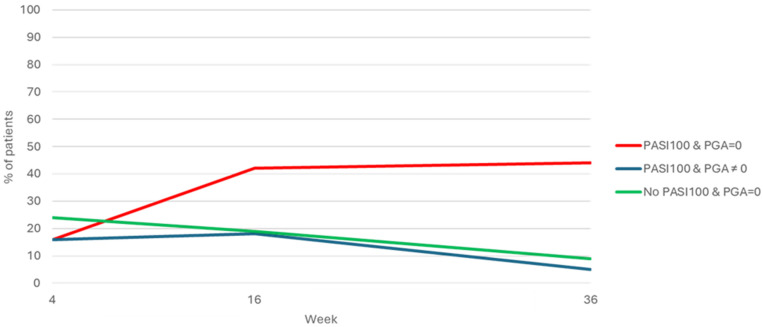
- DOI: 10.3390/ph17101378
Fast Clinical Response of Bimekizumab in Nail Psoriasis: A Retrospective Multicenter 36-Week Real-Life Study
Abstract
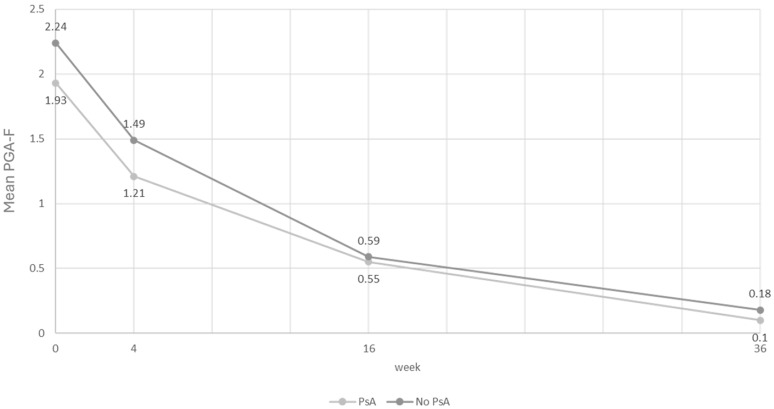
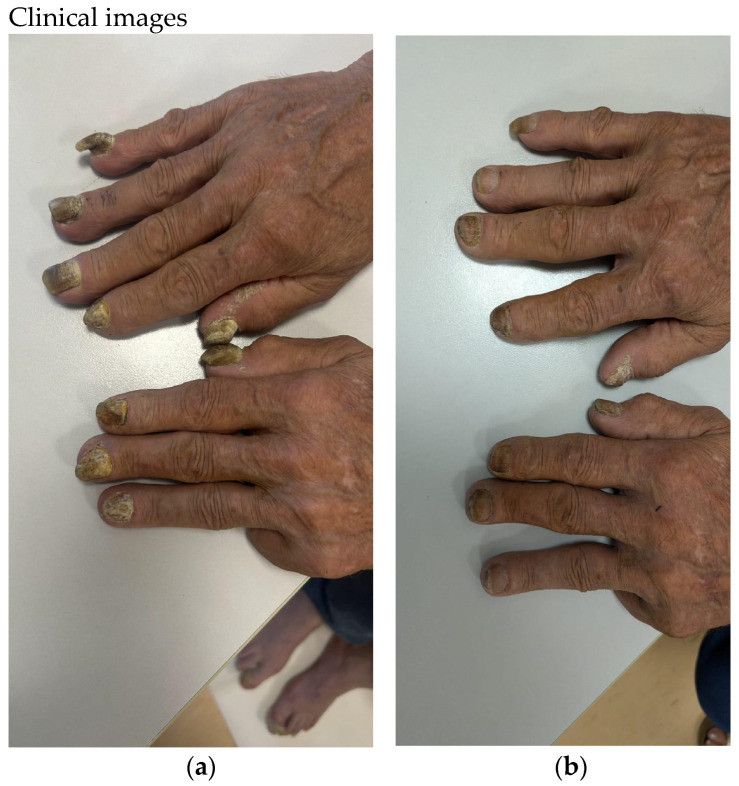
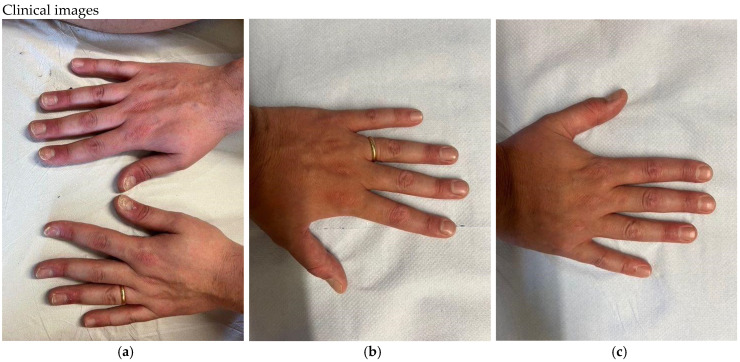
(1) Background/Objectives: Nail psoriasis (NP) is a chronic and difficult-to-treat disease, which causes significant social stigma and impairs the patients' quality of life. Moreover, nail psoriasis is a true therapeutic challenge for clinicians. The presence of nail psoriasis can be part of a severe form of psoriasis and can have predictive value for the development of psoriatic arthritis. Our real-world-evidence multicenter study aims to evaluate the efficacy of bimekizumab in nail psoriasis. (2) Methods: A retrospective analysis of a multicenter observational study included 834 patients affected by moderate-to-severe psoriasis, in 33 Dermatologic Units in Italy, treated with bimekizumab from December 2022 to September 2023. Clinimetric assessments were based on Psoriasis Area and Severity Index (PASI), Dermatology Life Quality Index (DLQI), and Physician's Global Assessment of Fingernail Psoriasis (PGA-F) for the severity of nail psoriasis at 0, 12, 24, and 36 weeks. (3) Results: Psoriatic nail involvement was present in 27.95% of patients. The percentage of patients who achieved a complete clearance of NP in terms of PGA-F 0 was 31.7%, 57%, and 88.5% at week 4, 16, and 36, respectively. PASI 100 was achieved by 32.03% of patients at week 4, by 61.8% at week 16, and by 78.92% of patients at week 36. The mean baseline PASI was 16.24. The mean DLQI values for the entire group of patients at baseline, at week 4, at week 16, and at week 36 were 14.62, 3.02, 0.83, and 0.5, respectively. (4) Conclusions: Therapies that promote the healing of both the skin and nails in a short time can also ensure a lower risk of subsequently developing arthritis which is disabling over time. Bimekizumab proved to be particularly effective to treat NP, with a fast response in terms of complete clearance, with over 88.5% of patients free from NP after 36 weeks. The findings of our real-world study showed that patients with moderate-to-severe PsO and concomitant NP had significantly faster and more substantial improvements in NP up to 36 weeks with respect to previous research findings. Considering the rapid healing of the nail, the dual inhibition of IL17 A and F might have a great value in re-establishing the dysregulation of keratin 17 at the nail level.
Keywords: PASI; PGA-F; bimekizumab; interleukin 17; nail psoriasis; psoriasis.
Conflict of interest statement
E. Campione has served as advisory board member and received fees for lectures and/or research grants by Almirall, Amgen, Abbvie, Bristol Myers Squibb, Incyte, Leo Pharma, and UCB. F. Artosi declares no conflicts of interest. R.Gaeta Shumack declares no conflicts of interest. A. Giunta has received grants and has been a consultant and speaker for AbbVie, Almirall, Celgene, Janssen, Leo Pharma, Eli Lilly, Merck Sharpe Dohme, Novartis, Pfizer, Sandoz, and UCB. L. Bianchi has served as speaker and consultant for AbbVie, Novartis, Janssen-Cilag, Pfizer, UCB, and LeoPharma. D. Orsini has been a speaker and/or consultant for Abbvie, LeoPharma, UCB, Bristol-Meyer-Squibb, and Boehringer-Ingelheim. P. Malagoli has been a speaker for AbbVie, Lilly, Novartis, Janssen-Cilag, Celgene, Leopharma, and Almirall. A. Balato has received honoraria for participation in advisory boards and meetings, or as speaker for AbbVie, Celgene, Janssen-Cilag, Eli Lilly, Novartis Pharma, Pfizer, Sanofi-Genzyme, and UCB Pharma. G. Caldarola reports consulting fees or honorarium and payment for lectures from Lilly and Novartis. A. Narcisi has served on advisory boards and received honoraria for lectures and research grants from Almirall, Abbvie, Leo Pharma, Celgene, Eli Lilly, Janssen, Novartis, Sanofi-Genzyme, Amgen, and Boehringer Ingelheim. A. Offidani has acted as a speaker and consultant for Abbvie, Eli Lilly, Novartis, Celgene, Sanofi, Galderma, Leo Pharma, and Pierre Fabre. A. Costanzo has served as advisory board member and consultant and received fees and speaker’s honoraria or participated in clinical trials for Abbvie, Almirall, Biogen, LEO Pharma, Lilly, Janssen, Novartis, Pfizer, Sanofi Genzyme, and UCB-Pharma. F. Loconsole declares no conflicts of interest. E. Mortato declares no conflicts of interest. M. Megna has acted as a speaker or consultant for Abbvie, Almirall, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Leo Pharma, Janssen, Novartis, Sandoz, and UCB. L. Gargiulo has been a consultant and/or speaker and participated in advisory boards for Abbvie, Almirall, Eli Lilly, Pfizer, Sanofi, and UCB Pharma. A. Carugno has been a consultant and/or speaker for Abbvie, Almirall, Amgen, Boehringer Ingelheim, Eli Lilly, Leo Pharma, Janssen-Cilag, Novartis, and UCB Pharma. V. Di Lernia has served as consultant and/or member of Data Safety Monitoring Boards or advisory boards and/or received speaker honoraria from Abbvie, Amgen, Eli Lilly, Janssen, and Novartis. A.V. Marzano has received consulting fees and disease-relevant honoraria from ABBVIE, AMGEN, BOEHRINGER INGELHEIM, BMS, INCYTE, LEOPHARMA, Novartis, Pfizer, SANOFI, and UCB. D. Strippoli has been a consultant and/or speaker for Almirall. Amgen, Janssen-Cilag, Sun-Pharma, Leo Pharma, Novartis, and UCB Pharma. G. Paolino has been a consultant for Abbvie, Pierre-Fabre, Janssen-Cilag, and Almirall. S. Lembo has acted as a speaker or consultant for Abbvie, Almirall, Eli Lilly, Leo Pharma, Janssen, Novartis, UCB, Sanofi, and Pfizer. M. Esposito has served as speaker and/or consultant for AbbVie, Almirall, Biogen, Celgene, Eli Lilly, Janssen, Leo Pharma, Novartis, Sanofi Genzyme, and UCB. M. C. Fargnoli has served on advisory boards and received honoraria for lectures and/or research grants from Amgen, Almirall, Abbvie, Boehringer-Ingelheim, BMS, Galderma, Kyowa Kyrin, Incyte, LEO Pharma, Pierre Fabre, UCB, Lilly, Pfizer, Janssen, MSD, Novartis, Sanofi, Regeneron, and Sun Pharma. A. Dattola has served as a speaker, consultant, or advisory board member for Abbvie, Almirall, Amgen, Eli Lilly, Leo Pharma, Janssen, Novartis, Boehringer Ingelheim, and UCB Pharma outside the submitted work. G.Pellacani has served as advisory board member for Abbvie, Almirall, Amgen, Leo Pharma, Janssen, Novartis, Canfield, Galderma, Lorèal, Sanofi, and UCB Pharma outside the submitted work. C.S. Fiorella has acted as a speaker or consultant for Abbvie, Almirall, Amgen, Eli Lilly, Leo Pharma, Janssen, Novartis, and UCB Pharma. E.Errichetti has been a consultant/speaker for Eli Lilly, Abbvie, Almirall, Amgen, LeoPharma, Janssen, Novartis, and UCB Pharma. M. Donini has been a consultant/speaker for Almirall, Leopharma, Novartis, Eli-Lilly, Abbvie, and Sanofi. P. Gisondi has served as a speaker, consultant, or advisory board member for Abbvie, Almirall, Amgen, Eli Lilly, Janssen, Leo Pharma, Novartis, Pierre Fabre, Sanofi, Sandoz, and UCB Pharma. E. Trovato declares no conflicts of interest. M.L. Musumeci has served as consultant and advisory board member and has participated in clinical trials for Janssen-Cilag, AbbVie, Almirall, Leo Pharma, Eli-Lilly, Novartis, Sanofi, UCB, and Boehringer-Ingelheim. C. De Simone has received honoraria from Amgen, Almirall, Abbvie, Boehringer-Ingelheim, Eli Lilly Incyte, LEO Pharma, UCB, Pfizer, Janssen, Novartis, and Sanofi, for serving as advisory board member, consultant, and/or speaker. F. Prignano has served as advisory board member and consultant and has received fees and speaker’s honoraria or has participated in clinical trials for AbbVie, Almirall, Leo Pharma, Eli-Lilly, Janssen, Novartis, Biogen, Sanofi Genzyme, UCB, and Boehringer-Ingelheim. M. Venturini has served as advisory board member and/or consultant and has received fees/speaker’s honoraria and/or has participated in clinical trials for AbbVie, Almirall, Amgen, Bristol Myers Squibb, Boehringer-Ingelheim, Eli Lilly, Galderma, Janssen, Leo Pharma, Novartis, Pierre Fabre, and UCB Pharma. No other disclosures have been made.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
