

Optimal Targeted Temperature Management for Patients with Post-Cardiac Arrest Syndrome
- PMID: 39459362
- PMCID: PMC11509509
- DOI: 10.3390/medicina60101575
Optimal Targeted Temperature Management for Patients with Post-Cardiac Arrest Syndrome
Abstract
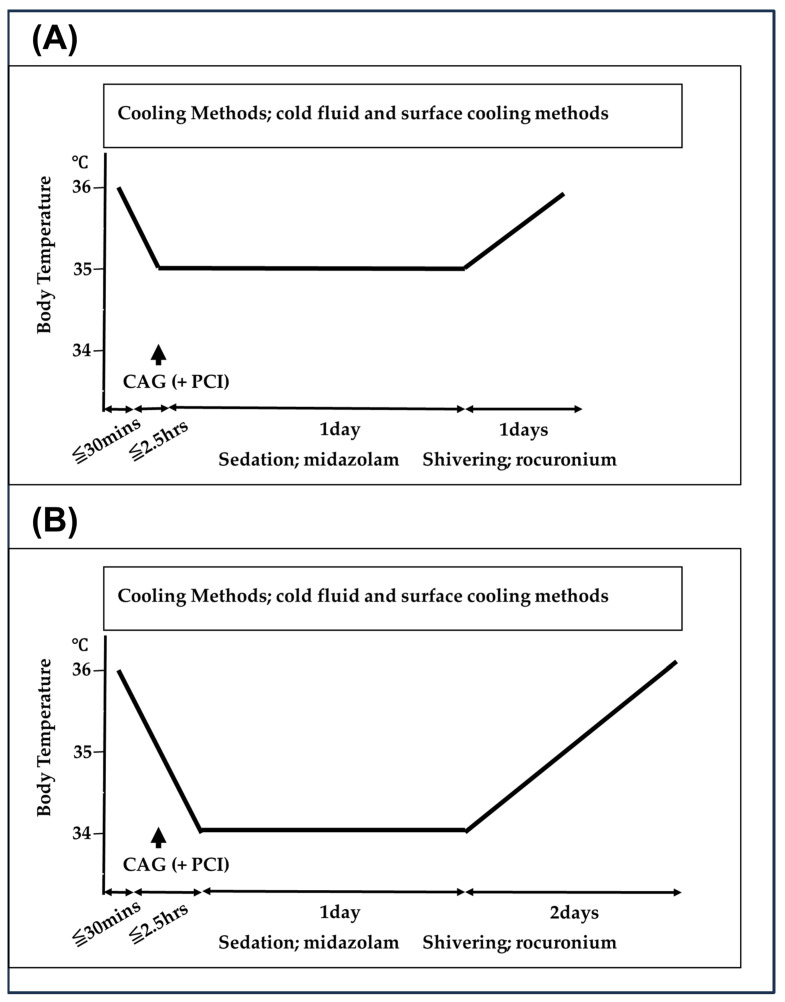
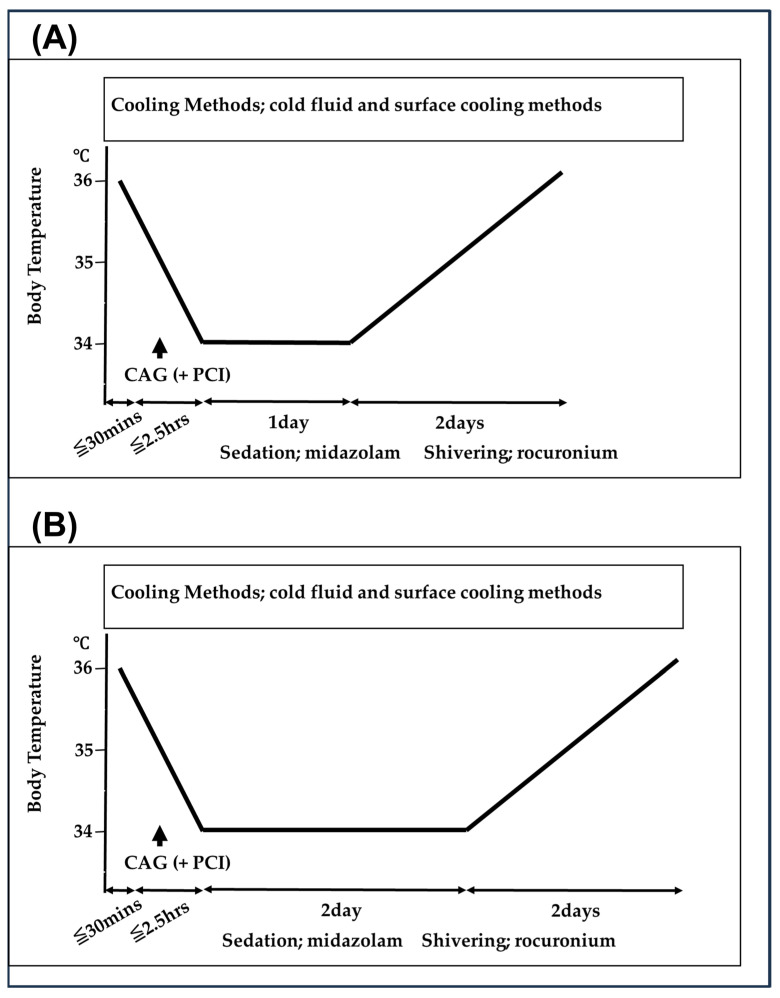
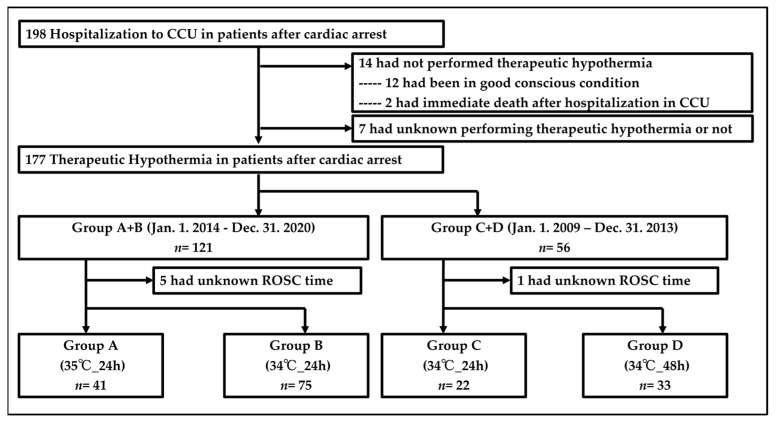
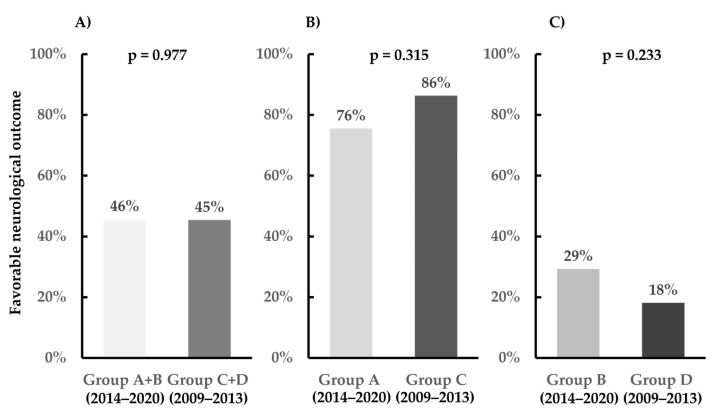
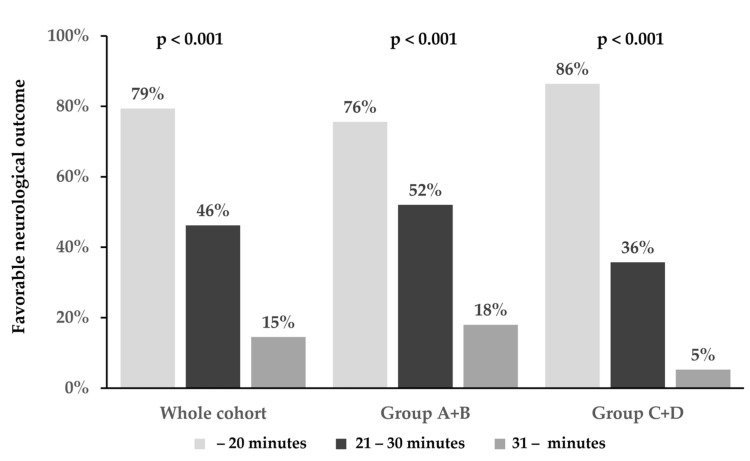
Background: To prevent hypoxic-ischemic brain damage in patients with post-cardiac arrest syndrome (PCAS), international guidelines have emphasized performing targeted temperature management (TTM). However, the most optimal targeted core temperature and cooling duration reached no consensus to date. This study aimed to clarify the optimal targeted core temperature and cooling duration, selected according to the time interval from collapse to return of spontaneous circulation (ROSC) in patients with PCAS due to cardiac etiology. Methods: Between 2014 and 2020, the targeted core temperature was 34 °C or 35 °C, and the cooling duration was 24 h. If the time interval from collapse to ROSC was within 20 min, we performed the 35 °C targeted core temperature (Group A), and, if not, we performed the 34 °C targeted core temperature (Group B). Between 2009 and 2013, the targeted core temperature was 34 °C, and the cooling duration was 24 or 48 h. If the interval was within 20 min, we performed the 24 h cooling duration (Group C), and, if not, we performed the 48 h cooling duration (Group D). Results: The favorable neurological outcome rates at 30 days following cardiac arrest were 45.7% and 45.5% in Groups A + B and C + D, respectively (p = 0.977). In patients with ROSC within 20 min, the favorable neurological outcome rates at 30 days following cardiac arrest were 75.6% and 86.4% in Groups A and C, respectively (p = 0.315). In patients with ROSC ≥ 21 min, the favorable neurological outcome rates at 30 days following cardiac arrest were 29.3% and 18.2% in Groups B and D, respectively (p = 0.233). Conclusions: Selecting the optimal target core temperature and the cooling duration for TTM, according to the time interval from collapse to ROSC, may be helpful in patients with PCAS due to cardiac etiology.
Keywords: post-cardiac arrest syndrome; resuscitation; targeted temperature management; therapeutic hypothermia.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Nolan J.P., Maconochie I., Soar J., Olasveengen T.M., Greif R., Wyckoff M.H., Singletary E.M., Aickin R., Berg K.M., Mancini M.E., et al. Executive Summary: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2020;142:s2–s27. doi: 10.1161/CIR.0000000000000890. - DOI - PubMed
-
- Merchant R.M., Topjian A.A., Panchal A.R., Cheng A., Aziz K., Berg K.M., Lavonas E.J., Magid D.J. Part 1: Executive Summary: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142:S337–S357. doi: 10.1161/CIR.0000000000000918. - DOI - PubMed
-
- Wyckoff M.H., Greif R., Morley P.T., Ng K.C., Olasveengen T.M., Singletary E.M., Soar J., Cheng A., Drennan I.R., Liley H.G., et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2022;146:e483–e557. doi: 10.1161/cir.0000000000001095. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
