

The Cardiometabolic Risk in Women with Polycystic Ovarian Syndrome (PCOS): From Pathophysiology to Diagnosis and Treatment
- PMID: 39459443
- PMCID: PMC11509436
- DOI: 10.3390/medicina60101656
The Cardiometabolic Risk in Women with Polycystic Ovarian Syndrome (PCOS): From Pathophysiology to Diagnosis and Treatment
Abstract
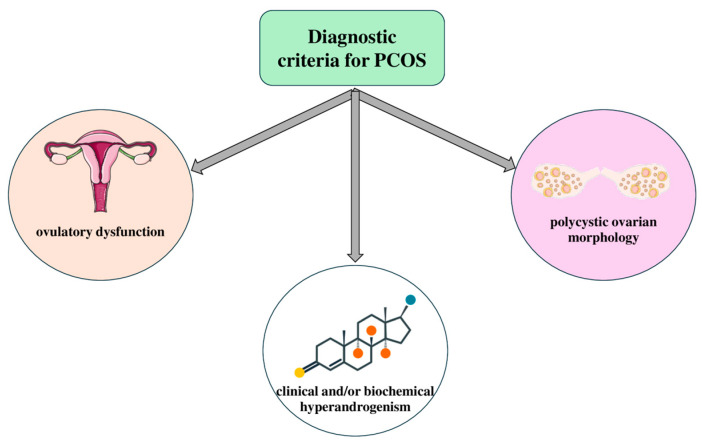
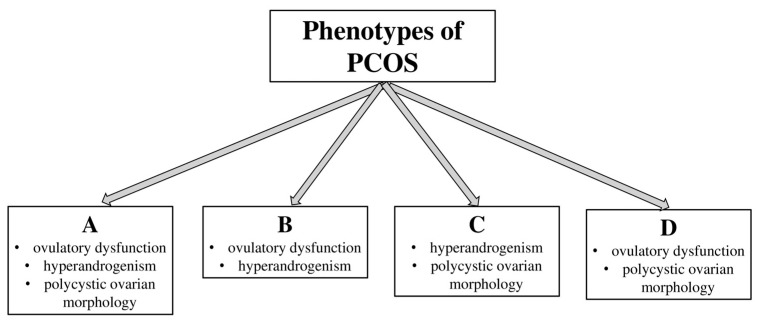
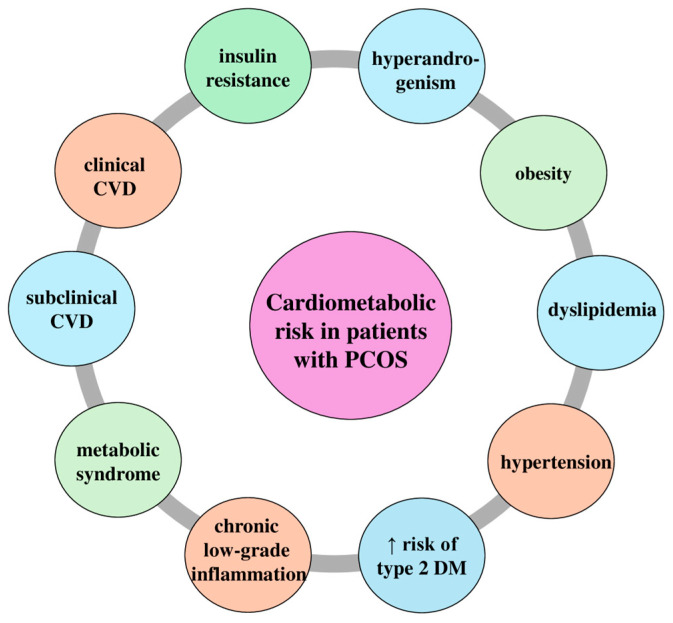
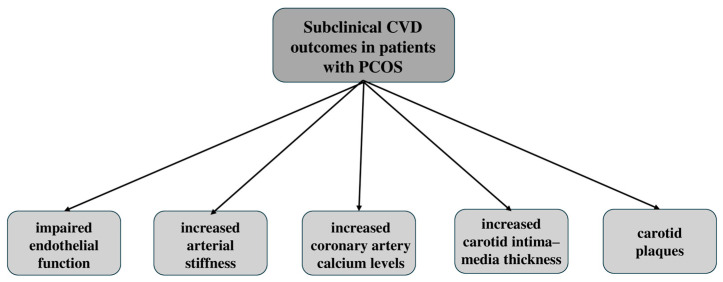
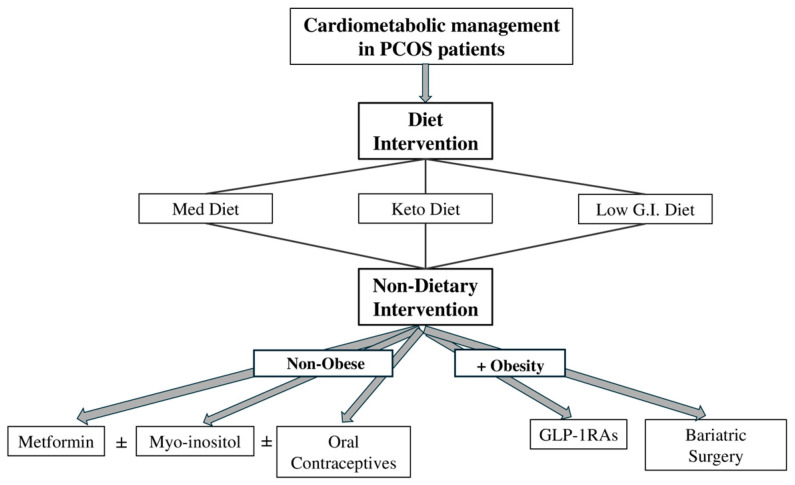
Polycystic Ovarian Syndrome (PCOS) is a prevalent endocrine disorder affecting women of reproductive age, with significant variations in presentation characterized by hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology. Beyond reproductive health, it may also pose crucial long-term cardiometabolic risks, especially for women with specific types of PCOS, contributing to early subclinical cardiovascular atherosclerotic alterations such as endothelial dysfunction, increased arterial stiffness, and coronary artery calcium levels, respectively. Moreover, the precise relationship between clinical cardiovascular disease (CVD) and PCOS remains debated, with studies demonstrating an elevated risk while others report no significant association. This review investigates the pathophysiology of PCOS, focusing on insulin resistance and its link to subclinical and clinical cardiovascular disease. Diagnostic challenges and novel management strategies, including lifestyle interventions, medications like metformin and glucagon-like peptide-1 receptor agonists (GLP-1RAs), hormonal contraceptives, and bariatric surgery, are further discussed. Recognizing the cardiometabolic risks associated with PCOS, a comprehensive approach and early intervention should address both the reproductive and cardiometabolic dimensions of the syndrome.
Keywords: cardiovascular disease; metabolic syndrome; polycystic ovarian syndrome; risk factors; treatment.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Andrews M.C. Bilateral polycystic ovaries associated with sterility, amenorrhea and hirsutism. Va. Med. Mon. 1952;79:544–548. - PubMed
-
- Diamanti-Kandarakis E., Kouli C.R., Bergiele A.T., Filandra F.A., Tsianateli T.C., Spina G.G., Zapanti E.D., Bartzis M.I. A survey of the polycystic ovary syndrome in the Greek island of Lesbos: Hormonal and metabolic profile. J. Clin. Endocrinol. Metab. 1999;84:4006–4011. doi: 10.1210/jcem.84.11.6148. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
