

Practice Guideline
doi: 10.1016/j.esmoop.2024.103664.
Epub 2024 Oct 1.
Neuroendocrine neoplasms of head and neck, genitourinary and gynaecological systems, unknown primaries, parathyroid carcinomas and intrathyroid thymic neoplasms: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up
Affiliations
- PMID: 39461777
- PMCID: PMC11549527
- DOI: 10.1016/j.esmoop.2024.103664
Item in Clipboard
Practice Guideline
Neuroendocrine neoplasms of head and neck, genitourinary and gynaecological systems, unknown primaries, parathyroid carcinomas and intrathyroid thymic neoplasms: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up
ESMO Open.
2024 Oct.
Abstract
- •
This Clinical Practice Guideline provides key recommendations for managing rare endocrine tumours.
- •
Neuroendocrine neoplasms of different origins, parathyroid carcinoma and intrathyroid thymic neoplasms are included.
- •
The guideline covers clinical imaging and pathological diagnosis, staging and risk assessment, treatment and follow-up.
- •
The authors comprise a multidisciplinary group of experts from different institutions and countries in Europe.
- •
Recommendations are based on available scientific data and the authors’ collective expert opinion.
Keywords: ESMO guideline; diagnosis; intrathyroid carcinoma; management; parathyroid carcinoma; rare endocrine neoplasms.
Figures
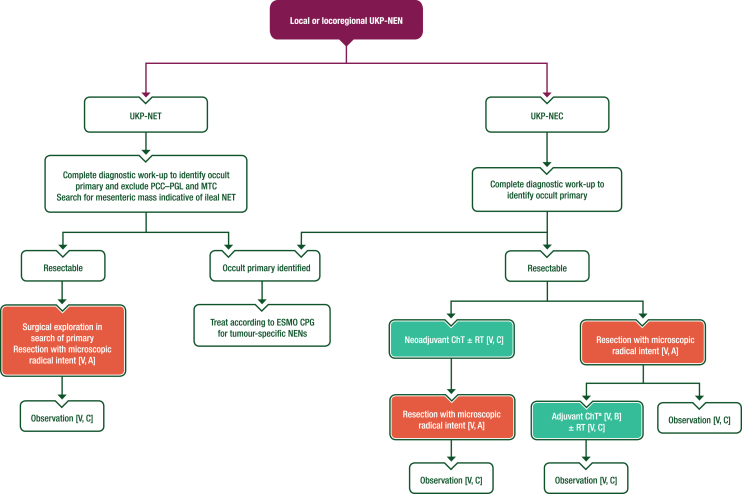
Management of local or locoregional UKP-NENs. Purple: algorithm title; orange: surgery; turquoise: non-systemic anticancer therapies or combination of treatment modalities; white: other aspects of management and non-treatment aspects. ChT, chemotherapy; CPG, Clinical Practice Guideline; MTC, medullary thyroid cancer; NEC, neuroendocrine carcinoma; NEN, neuroendocrine neoplasm; NET, neuroendocrine tumour; PCC–PGL, pheochromocytoma–paraganglioma; RT, radiotherapy; UKP, unknown primary. aFour cycles of platinum–etoposide.
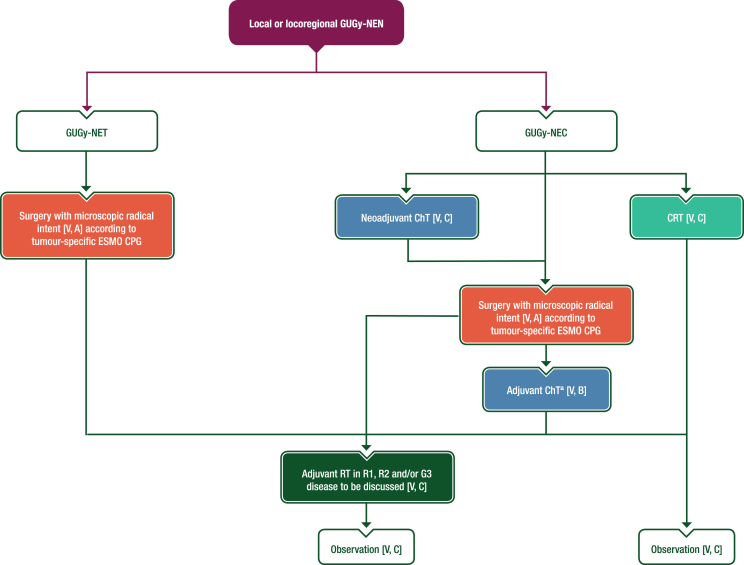
Management of local or locoregional GUGy-NENs. Purple: algorithm title; orange, surgery; dark green: RT; blue: systemic anticancer therapy or their combination; turquoise: non-systemic anticancer therapies or combination of treatment modalities; white: other aspects of management and non-treatment aspects. ChT, chemotherapy; CPG, Clinical Practice Guideline; CRT, chemoradiotherapy; G, grade; GUGy, genitourinary or gynaecological; NEC, neuroendocrine carcinoma; NEN, neuroendocrine neoplasm; NET, neuroendocrine tumour; R1, resection with microscopic tumour at the margin; R2, resection with macroscopic tumour at the margin; RT, radiotherapy. aFour cycles of platinum–etoposide.
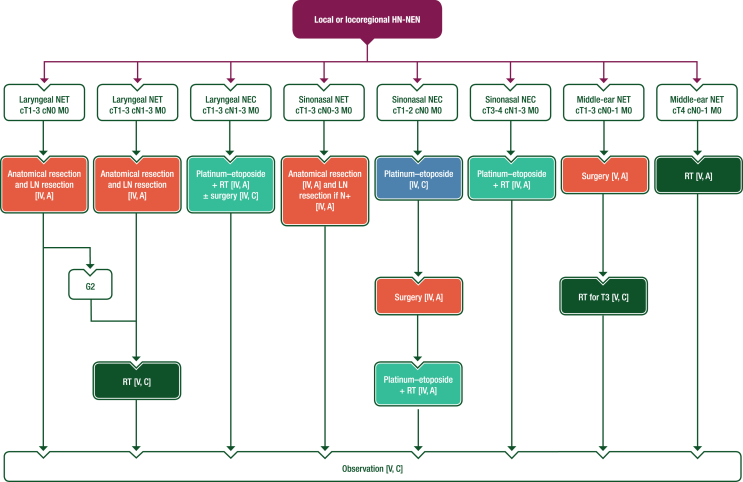
Management of local or locoregional HN-NENs. Purple: algorithm title; orange: surgery; dark green: RT; blue: systemic anticancer therapy or their combination; turquoise: non-systemic anticancer therapies or combination of treatment modalities; white: other aspects of management and non-treatment aspects. c, clinical; G, grade; HN, head and neck; LN, lymph node; M, metastasis; N, node; N+, lymph node metastasis; NEC, neuroendocrine carcinoma; NEN, neuroendocrine neoplasm; NET, neuroendocrine tumour; RT, radiotherapy; T, tumour.
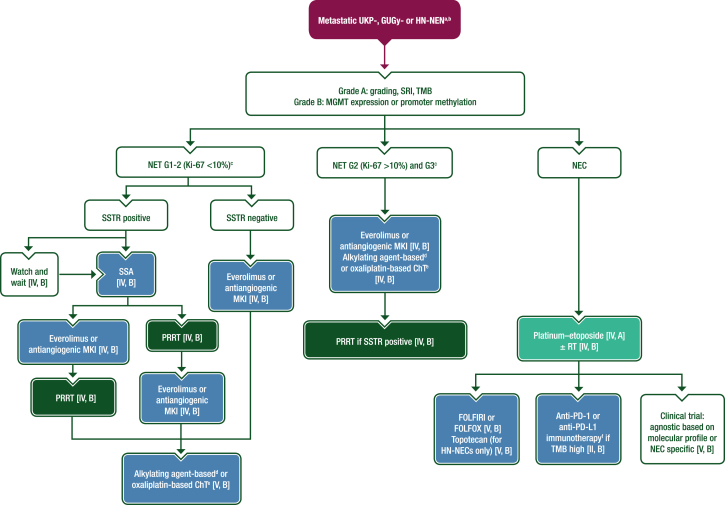
Management of metastatic UKP-, GUGy- and HN-NENs. Purple: algorithm title; dark green: RT; blue: systemic anticancer therapy or their combination; turquoise: non-systemic anticancer therapies or combination of treatment modalities; white: other aspects of management and non-treatment aspects. 5-FU, 5-fluorouracil; ChT, chemotherapy; EMA, European Medicines Agency; FDA, Food and Drug Administration; FOLFIRI, leucovorin–5-fluorouracil–irinotecan; FOLFOX, leucovorin–5-fluorouracil–oxaliplatin; G, grade; GUGy, genitourinary or gynaecological; HN, head and neck; MGMT, O-6-methylguanine-DNA methyltransferase; MKI, multikinase inhibitor; NEC, neuroendocrine carcinoma; NEN, neuroendocrine neoplasm; NET, neuroendocrine tumour; PD-1, programmed cell death protein 1; PD-L1, programmed death-ligand 1; PRRT, peptide receptor radionuclide therapy; R0, resection with no tumour at the margin; RT, radiotherapy; SRI, somatostatin receptor imaging; SSA, somatostatin analogue; SSTR, somatostatin receptor; TMB, tumour mutational burden; UKP, unknown primary. aAlways consider enrolment in a clinical trial [V, A]. bRecommendations for the management of metastatic UKP-, GUGy- and HN-NENs are based on the management of NENs of GEP or lung origin and therefore systemic treatments approved for GEP-NETs are used off-label in these settings. cSurgery is recommended if disease is amenable to R0 resection [V, A]. dDacarbazine, temozolomide or streptozocin plus 5-FU or capecitabine. eOxaliplatin plus 5-FU or capecitabine. fPembrolizumab is FDA approved (but not EMA approved) for the treatment of patients with unresectable or metastatic TMB high solid tumours that have progressed following prior treatment and have no alternative treatment options. No other anti-PD-1 or anti-PD-L1 agents are approved for use in patients with TMB high solid tumours.
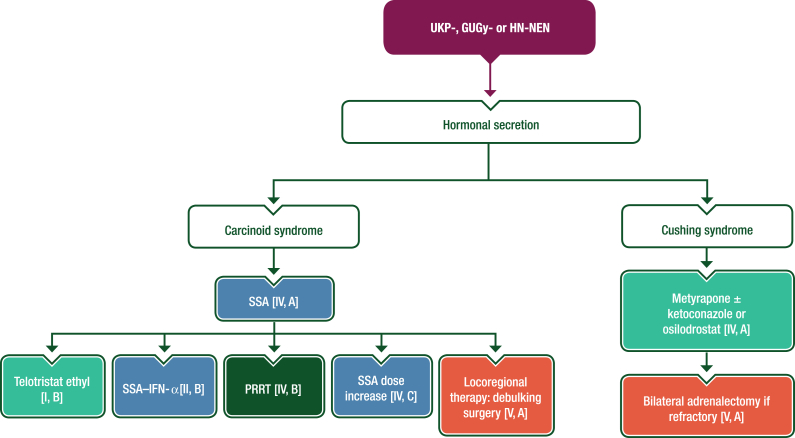
Management of carcinoid syndrome and Cushing syndrome induced by UKP-, GUGy- or HN-NENs. Purple: algorithm title; orange: surgery; dark green: RT; blue: systemic anticancer therapy or their combination; turquoise: non-systemic anticancer therapies or combination of treatment modalities; white: other aspects of management and non-treatment aspects. GUGy, genitourinary or gynaecological; HN, head and neck; IFN-α, interferon-α; NEN, neuroendocrine neoplasm; PRRT, peptide receptor radionuclide therapy; SSA, somatostatin analogue; UKP, unknown primary.
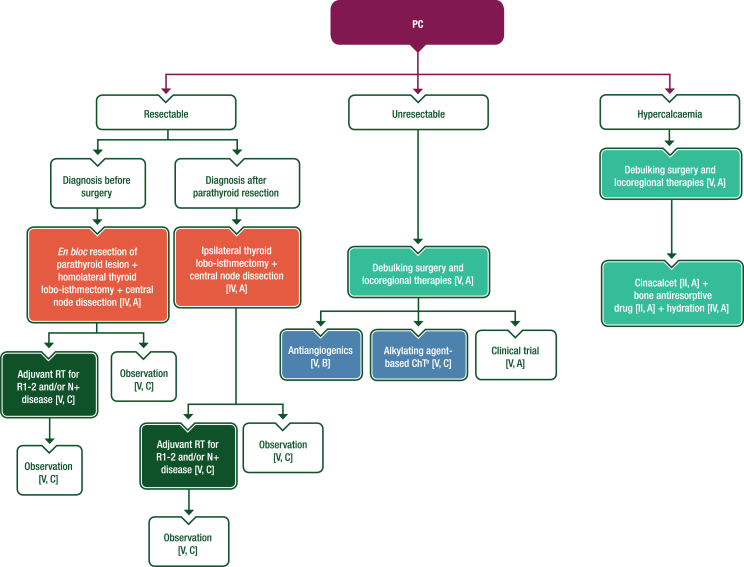
Management of PC. Purple: algorithm title; orange: surgery; dark green: RT; blue: systemic anticancer therapy or their combination; turquoise: non-systemic anticancer therapies or combination of treatment modalities; white: other aspects of management and non-treatment aspects. 5-FU, 5-fluorouracil; ChT, chemotherapy; N+, lymph node metastasis; PC, parathyroid carcinoma; R1, resection with microscopic tumour at the margin; R2, resection with macroscopic tumour at the margin; RT, radiotherapy. aDacarbazine, temozolomide or streptozocin plus 5-FU or capecitabine.
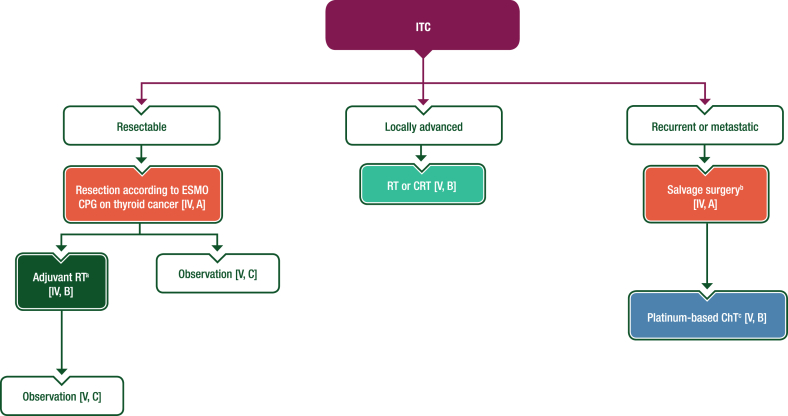
Management of ITC. Purple: algorithm title; orange: surgery; dark green: RT; blue: systemic anticancer therapy or their combination; turquoise: non-systemic anticancer therapies or combination of treatment modalities; white: other aspects of management and non-treatment aspects. ChT, chemotherapy; CPG, clinical practice guideline; CRT, chemoradiotherapy; ITC, intrathyroid thymic carcinoma; MTB, multidisciplinary tumour board; RT, radiotherapy. aIn selected cases after careful MTB discussion. bAdjuvant RT may be discussed for patients who have not received prior RT [V, B]. cCisplatin-based regimens with either doxorubicin and cyclophosphamide or etoposide.
References
-
- Hadoux J., Kanaan C., Durand A., et al. Prognostic factors of metastatic neuroendocrine carcinoma under first-line treatment with platinum etoposide with a focus on NEC score and Rb expression: results from the multicentre RBNEC study of the Groupe d'Etude des Tumeurs Endocrines (GTE) and the ENDOCAN-RENATEN network. Eur J Cancer. 2021;152:100–115. - PubMed
-
- Pósfai B., Kuthi L., Varga L., et al. The colorful palette of neuroendocrine neoplasms in the genitourinary tract. Anticancer Res. 2018;38(6):3243–3254. - PubMed
-
- van der Zwan J.M., Mallone S., van Dijk B., et al. Carcinoma of endocrine organs: results of the RARECARE project. Eur J Cancer. 2012;48(13):1923–1931. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
