

The prognostic impact of maximal aortic diameter on acute type B aortic dissection progression in a Chinese population
- PMID: 39462034
- PMCID: PMC11513997
- DOI: 10.1038/s41598-024-77649-3
The prognostic impact of maximal aortic diameter on acute type B aortic dissection progression in a Chinese population
Abstract
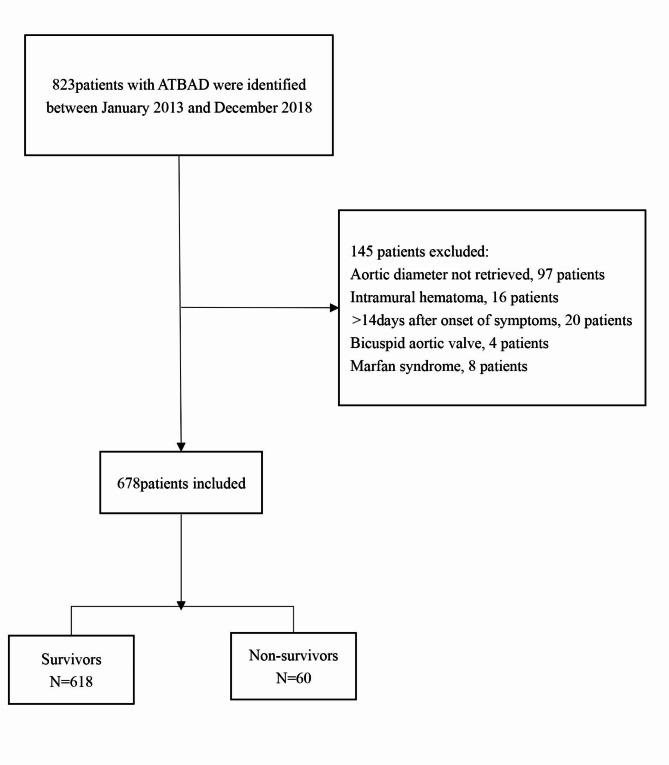
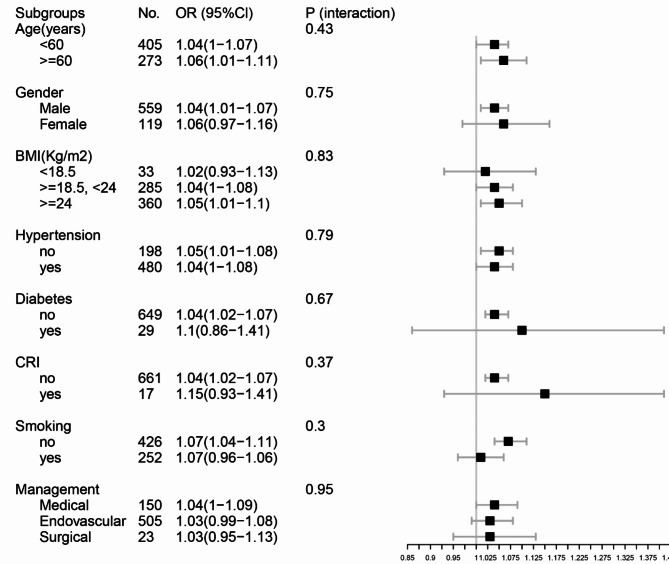
Currently, evidence concerning the link between maximal aortic diameter and in-hospital mortality in cases of acute type B aortic dissection (ATBAD) is insufficient. Thus, this study aimed to explore the relationship between the maximal aortic diameter at the time of admission and the early prognosis of patients diagnosed with ATBAD. A total of 678 patients with ATBAD were included between January 2016 and December 2018, during which their clinical data was gathered. The independent variable analyzed was the maximal diameter of the aorta, while the dependent variable was mortality during hospitalization. Factors considered in this analysis included the patients' age, gender, body mass index (BMI), medical history of hypertension, stroke, diabetes, atherosclerosis, smoking habits, chronic kidney insufficiency, time until presentation, systolic and diastolic blood pressures, ejection fraction, presence of aortic regurgitation, symptoms, involvement of abdominal vessels, laboratory findings, and treatment approaches. Of these patients collected, the mean age was 56.03 ± 12.22 years, and approximately 82.45% of them were male. After analysis, it was found that the maximal aortic diameter of patients with ATBAD was positively correlated with in-hospital mortality (OR = 1.06, 95% CI 1.03 to 1.10). Surprisingly, a J curve relationship was detected between maximal aortic diameter (point 31 mm) and in-hospital death for patients with ATBAD. The effect sizes and confidence intervals of the right (maximal aortic diameter > 31 mm) and left (maximal aortic diameter ≤ 31 mm) aspects of the inflection point were 1.06 (1.02-1.11) and 1.03 (0.83-1.28), respectively. In addition, the stratified analysis showed a stable relationship between maximal aortic diameter and in-hospital mortality, while there was no significant difference in the interaction between different subgroups. In patients with ATBAD, a J-curve relationship was identified between the maximal aortic diameter and in-hospital mortality. Specifically, when the maximal aortic diameter exceeds 31 mm, a positive correlation with in-hospital death was observed.
Keywords: Acute type B aortic dissection; In-hospital mortality; Maximal aortic diameter.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Tolenaar, J. L. et al. Predicting in-hospital mortality in acute type B aortic dissection: evidence from International Registry of Acute Aortic Dissection. Circulation. 130, S45–S50 (2014). - PubMed
MeSH terms
Grants and funding
- 2023JJ40867/Natural Science Foundation of Hunan Province
- B202310007057/Hunan Health and Family Planning Commission Project
- 202214053517/Hunan Health and Family Planning Commission Project
- kq2208330/Natural Science Foundation of Changsha
- 2019SK2022/The key Research and Development Program of Hunan Province
LinkOut - more resources
Full Text Sources
