

Impact of semaglutide on weight and functional outcomes among obese heart failure patients: a propensity scores matching analysis
- PMID: 39462311
- PMCID: PMC11515153
- DOI: 10.1186/s12872-024-04275-2
Impact of semaglutide on weight and functional outcomes among obese heart failure patients: a propensity scores matching analysis
Abstract
Background & objectives: Obesity is a common comorbidity in heart failure, yet effective pharmacological options for weight loss in these patients are limited. Semaglutide, a glucagon-like peptide 1 receptor agonist, has shown promise for weight reduction in obese adults. This study aims to evaluate semaglutide's impact on weight loss, functional status, and clinical outcomes in obese patients with heart failure.
Methods: A retrospective analysis was conducted on all consecutive obese (BMI > 30 kg/m²) patients with heart failure at the University Hospital Bonn outpatient clinic from July 2019 to July 2022. Propensity score matching paired patients receiving semaglutide as an add-on therapy (SEMA) with those on medical therapy alone (Control).
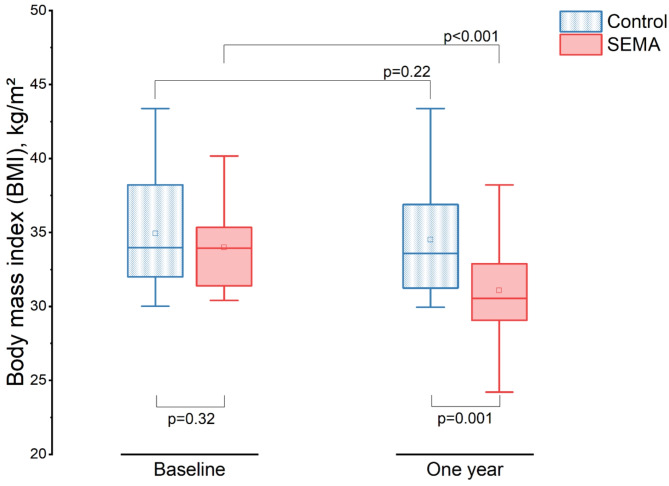
Results: Among 1,942 patients with heart failure screened, 26 matched pairs were identified. At one year, the SEMA group exhibited significant weight loss, with a mean BMI reduction of -2.91 kg/m² (95% CI: -4.27 to -1.55; p < 0.001), while the control group showed a non-significant mean change of -0.41 kg/m² (95% CI: -1.08 to 0.26; p = 0.22). The difference in BMI between the two groups was statistically significant (mean difference: 3.42 kg/m², 95% CI: 1.43 to 5.42; p = 0.001). Improvements by at least one NYHA class were observed in 65% of the SEMA group (p < 0.001) compared to 15% of the control group (p = 0.18). The SEMA group also showed a significant increase in 6-minute walk distance (6MWD), with a mean difference of 75 m between the groups at one year (95% CI: 0.53 to 150.02; p = 0.049). NT-proBNP levels significantly decreased in the SEMA group (p < 0.001) compared to the control group (p = 0.78), with a statistically significant difference in NT-proBNP between the groups (p = 0.048). Both improvements in 6MWD and reductions in NT-proBNP were significantly correlated with BMI percentage reductions.
Conclusions: Semaglutide was associated with significant weight reduction in obese patients with heart failure, accompanied by improved NYHA classification and 6-minute walk distance. Larger, multi-center trials and prospective, randomized controlled trials are warranted. These studies should focus on assessing long-term outcomes, optimizing dosage, and exploring the potential cardiovascular benefits beyond weight reduction.
Keywords: Glucagon-like peptide 1 receptor agonist; Heart failure; Semaglutide; Weight reduction.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
