

Cortical Venting: A Simple Surgical Adjunct for the Treatment of Long Bone Nonunion
- PMID: 39463543
- PMCID: PMC11506486
- DOI: 10.7759/cureus.70193
Cortical Venting: A Simple Surgical Adjunct for the Treatment of Long Bone Nonunion
Abstract
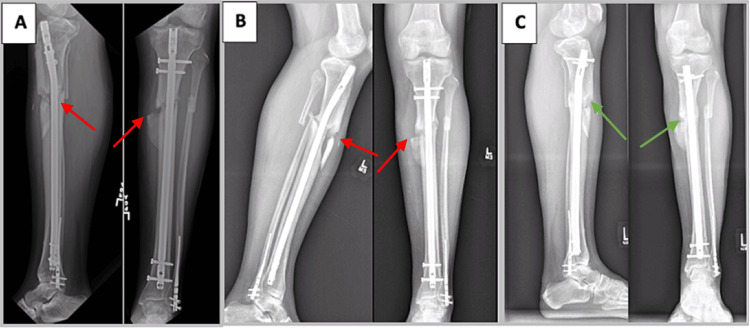
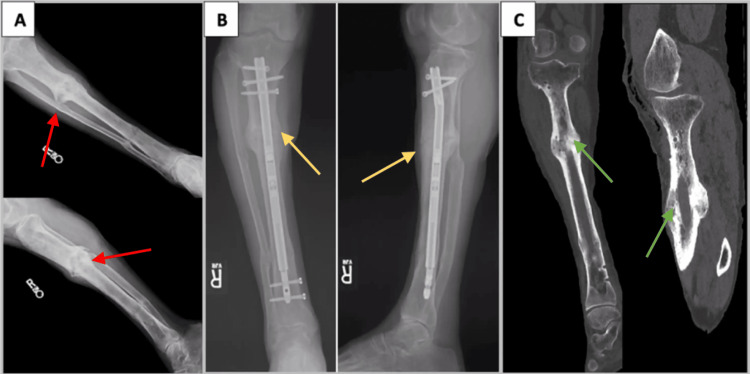
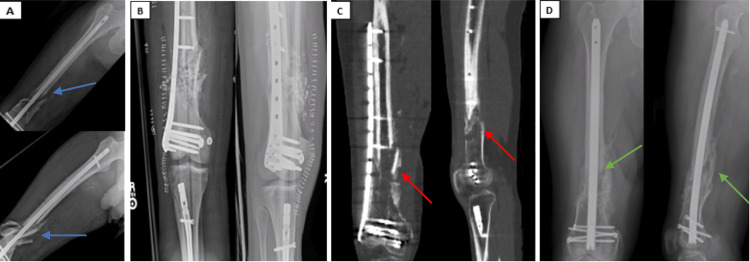
Nonunions are a vexing problem for the orthopedic surgeon. Herein, we describe an adjunct to the standard exchange nailing procedure adapted from an established limb lengthening technique in which cortical vents are drilled adjacent to the nonunion site. These transcortical drill tunnels facilitate local dispersion of the osteogenic intramedullary reamings around the nonunion site during the exchange nailing, whereby the extruded reamings serve as autograft for the nonunion. This simple adjunctive technique can increase the likelihood of achieving union when performed with an exchange nailing procedure as demonstrated by our case series of recalcitrant tibia and femoral nonunions successfully treated when this surgical adjunct was implemented.
Keywords: cortical venting; exchange nailing; long bone fractures; nonunion; orthopaedic trauma.
Copyright © 2024, Wade et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- Treatment of severely open tibial fractures, non-unions, and fracture-related infections with a gentamicin-coated tibial nail-clinical outcomes including quality of life analysis and psychological ICD-10-based symptom rating. Walter N, Popp D, Freigang V, Nerlich M, Alt V, Rupp M. J Orthop Surg Res. 2021;16:270. - PMC - PubMed
-
- Outcomes of patients with nonunion after open tibial shaft fractures with or without soft tissue coverage procedures. Egol KA, Littlefield CP, Walden T, Leucht P, Levine J, Konda S. J Orthop Trauma. 2021;35:0–6. - PubMed
-
- Path analysis of factors for delayed healing and nonunion in 416 operatively treated tibial shaft fractures. Audigé L, Griffin D, Bhandari M, Kellam J, Rüedi TP. Clin Orthop Relat Res. 2005;438:221–232. - PubMed
-
- Fractures of the tibia: can their outcome be predicted? Gaston P, Will E, Elton RA, McQueen MM, Court-Brown CM. J Bone Joint Surg Br. 1999;81:71–76. - PubMed
Publication types
LinkOut - more resources
Full Text Sources