

Abemaciclib combined with endocrine therapy as adjuvant treatment for hormone-receptor-positive, HER2-, high-risk early breast cancer: 5-year Chinese population analysis of the phase III randomized monarchE study
- PMID: 39463748
- PMCID: PMC11503738
- DOI: 10.1177/17588359241286775
Abemaciclib combined with endocrine therapy as adjuvant treatment for hormone-receptor-positive, HER2-, high-risk early breast cancer: 5-year Chinese population analysis of the phase III randomized monarchE study
Abstract
Background: Abemaciclib was the first cyclin-dependent kinase 4/6 (CDK4/6) inhibitor approved globally in the adjuvant setting for high-risk hormone-receptor positive (HR+)/human epidermal growth factor 2 negative (HER2-) early breast cancer (EBC), based on the phase III monarchE trial.
Objective: To report an exploratory Chinese population analysis based on the preplanned overall survival (OS) interim analysis with 5-year efficacy results of monarchE.
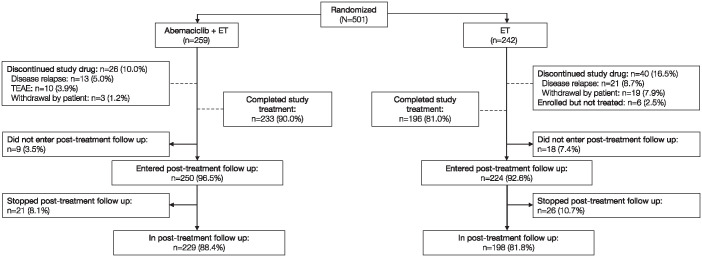
Design and methods: Patients with HR+/HER2-, high-risk (⩾4 positive lymph nodes, or 1-3 nodes and either tumor size ⩾5 cm, histologic grade 3, or Ki-67 ⩾20%) EBC were randomized (1:1) to abemaciclib (150 mg twice daily for 2 years) plus endocrine therapy (ET), or ET alone. This analysis included Chinese patients enrolled in mainland China, Hong Kong, and Taiwan. The primary endpoint was invasive disease-free survival (IDFS); key secondary endpoints included distant relapse-free survival (DRFS), safety, and patient-reported outcomes (PROs).
Results: Overall, 501 Chinese patients were included (abemaciclib + ET, n = 259; ET, n = 242). With a median follow-up of 53 months, the addition of abemaciclib to ET resulted in improvements in IDFS (estimated 5-year IDFS rate: 85.9% vs 79.1%; hazard ratio (HR), 0.65 (95% confidence interval (CI) 0.41-1.03)) and DRFS (estimated 5-year DRFS rate: 88.4% vs 82.3%; HR, 0.65 (95% CI, 0.39-1.07)). The most common grade ⩾3 treatment-emergent adverse events in the abemaciclib + ET versus ET groups were neutropenia (24.7% vs 0.8%) and leukopenia (22.4% vs 0.4%). Generally, no clinically meaningful difference in PROs (endocrine symptoms and fatigue) was observed between groups, except for diarrhea.
Conclusion: At this prespecified OS interim analysis, which provides 5-year data, the addition of abemaciclib to ET in Chinese patients with high-risk HR+, HER2- EBC was associated with sustained and clinically meaningful improvements in IDFS and DRFS, with acceptable safety and tolerability profiles and minimal impact on PROs. These results represent the first full report of a CDK4/6 inhibitor in Chinese patients with EBC and support the positive benefit-risk profile of adjuvant abemaciclib + ET in Chinese patients.
Trial registration: ClinicalTrials.gov identifier: NCT03155997 (first posted: May 16, 2017).
Keywords: Chinese; HR+/HER2−; abemaciclib; adjuvant; breast cancer.
© The Author(s), 2024.
Conflict of interest statement
L.Y. and C.Q. are employees of Eli Lilly and Company. The other authors declare they have no competing interests.
Figures


References
-
- Sung H, Ferlay J, Siegel RL, et al.. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209–249. - PubMed
-
- Fan L, Zheng Y, Yu KD, et al.. Breast cancer in a transitional society over 18 years: trends and present status in Shanghai, China. Breast Cancer Res Treat 2009; 117: 409–416. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
