

Diagnostic utility of prostate health index density prior to MRI-ultrasound fusion targeted biopsy
- PMID: 39465014
- PMCID: PMC11502073
- DOI: 10.37349/etat.2024.00269
Diagnostic utility of prostate health index density prior to MRI-ultrasound fusion targeted biopsy
Abstract
Aim: Prostate biopsy can be prone to complications and thus should be avoided when unnecessary. Although the combination of magnetic resonance imaging (MRI), the prostate health index (PHI), and PHI density (PHID) has been shown to improve detection of clinically significant prostate cancer (csPCa), there is limited information available assessing its clinical utility. We sought to determine whether using PHID could enhance the detection of PCa on MRI ultrasound fusion-targeted biopsy (MRF-TB) compared to other biomarker cutoffs.
Methods: Between June 2015 and December 2020, 302 men obtained PHI testing before MRF-TB at a single institution. We used descriptive statistics, multivariable logistic regression, and receiver operating characteristic curves to determine the predictive accuracy of PHID and PHI to detect ≥ Gleason grade group (GGG) 2 PCa and identify cutoff values.
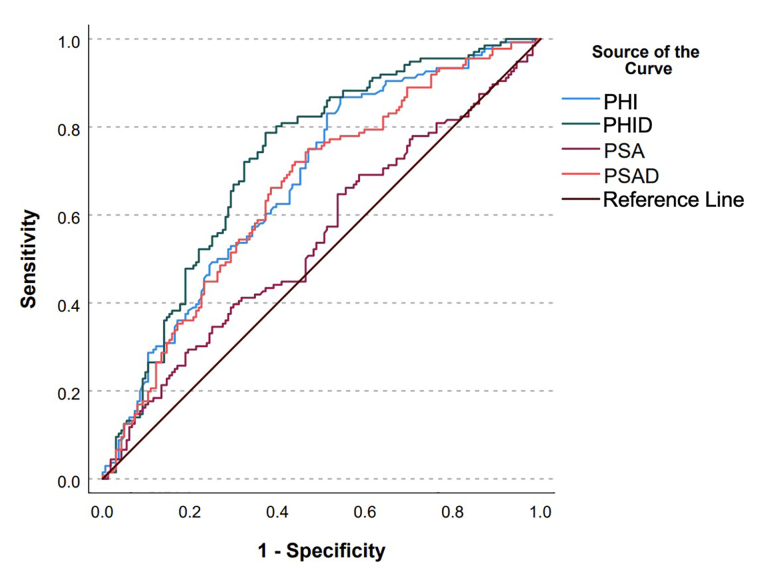
Results: Any cancer grade was identified in 75.5% of patients and ≥ GGG2 PCa was identified in 45% of patients. The median PHID was 1.05 [interquartile range (IQR) 0.59-1.64]. A PHID cutoff of 0.91 had a higher discriminatory ability to predict ≥ GGG2 PCa compared to PHI > 27, PHI > 36, and prostate specific-antigen (PSA) density > 0.15 (AUC: 0.707 vs. 0.549 vs. 0.620 vs. 0.601), particularly in men with Prostate Imaging Reporting and Data System (PI-RADS) 1-2 lesions on MRI (AUC: 0.817 vs. 0.563 vs. 0.621 vs. 0.678). At this cutoff, 35.0% of all the original biopsies could be safely avoided (PHID < 0.91 and no ≥ GGG2 PCa) and csPCa would be missed in 9.67% of patients who would have been biopsied. In patients with PI-RADS 1-2 lesions using a PHID cutoff of 0.91, 56.8% of biopsies could be safely avoided while missing 0 csPCa.
Conclusions: These findings suggest that a PHID cutoff of 0.91 improves the selection of patients with elevated prostate-specific antigen who are referred for prostate biopsy, and potentially in patients with PI-RADS 1-2 lesions.
Keywords: MRI; Prostatic neoplasms; image-guided biopsies; prostate-specific antigen; protein isoforms.
© The Author(s) 2024.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Catalona WJ, Richie JP, Ahmann FR, Hudson MA, Scardino PT, Flanigan RC, et al. Comparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6,630 men. J Urol. 1994;151:1283–90. doi: 10.1016/s0022-5347(17)35233-3. - DOI - PubMed
-
- Gretzer MB, Partin AW. PSA levels and the probability of prostate cancer on biopsy. Eur Urol Suppl. 2002;1:21–7. doi: 10.1016/S1569-9056(02)00053-2. - DOI
-
- Tadayon F, Arezegar HR, Khorrami MH, Hashemi Juzdani R, Shahdoost AA, Mellat M. Evaluation of prostatic cancer prevalence in patients with prostatic-specific antigen between 4 and 10 and normal digital rectal examination. Adv Biomed Res. 2016;5:112. doi: 10.4103/2277-9175.184298. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous