

Combined targeting of GPX4 and BCR-ABL tyrosine kinase selectively compromises BCR-ABL+ leukemia stem cells
- PMID: 39465372
- PMCID: PMC11514791
- DOI: 10.1186/s12943-024-02162-0
Combined targeting of GPX4 and BCR-ABL tyrosine kinase selectively compromises BCR-ABL+ leukemia stem cells
Abstract
Background: In the ongoing battle against BCR-ABL+ leukemia, despite significant advances with tyrosine kinase inhibitors (TKIs), the persistent challenges of drug resistance and the enduring presence of leukemic stem cells (LSCs) remain formidable barriers to achieving a cure.
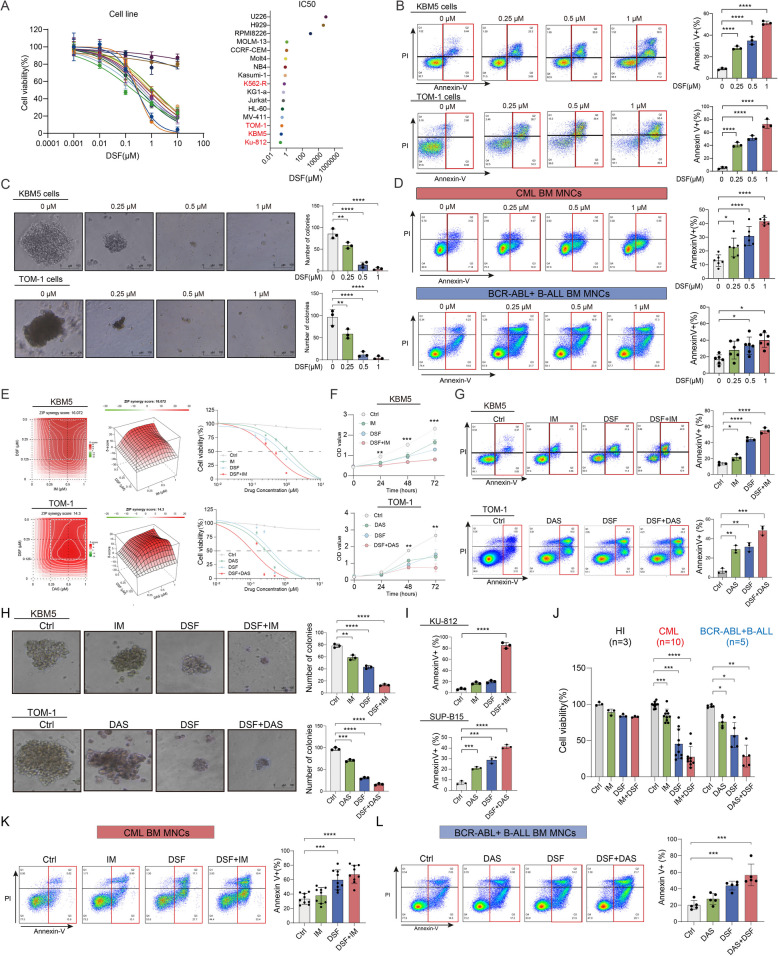
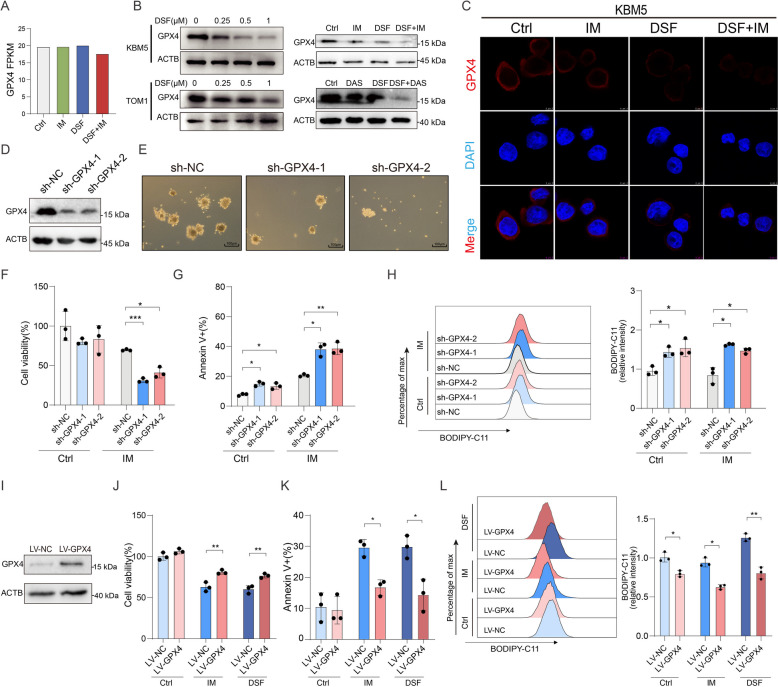
Methods: In this study, we demonstrated that Disulfiram (DSF) induces ferroptosis to synergize with TKIs in inhibiting BCR-ABL+ cells, particularly targeting resistant cells and LSCs, using cell models, mouse models, and primary cells from patients. We elucidated the mechanism by which DSF promotes GPX4 degradation to induce ferroptosis through immunofluorescence, co-immunoprecipitation (CO-IP), RNA sequencing, lipid peroxidation assays, and rescue experiments.
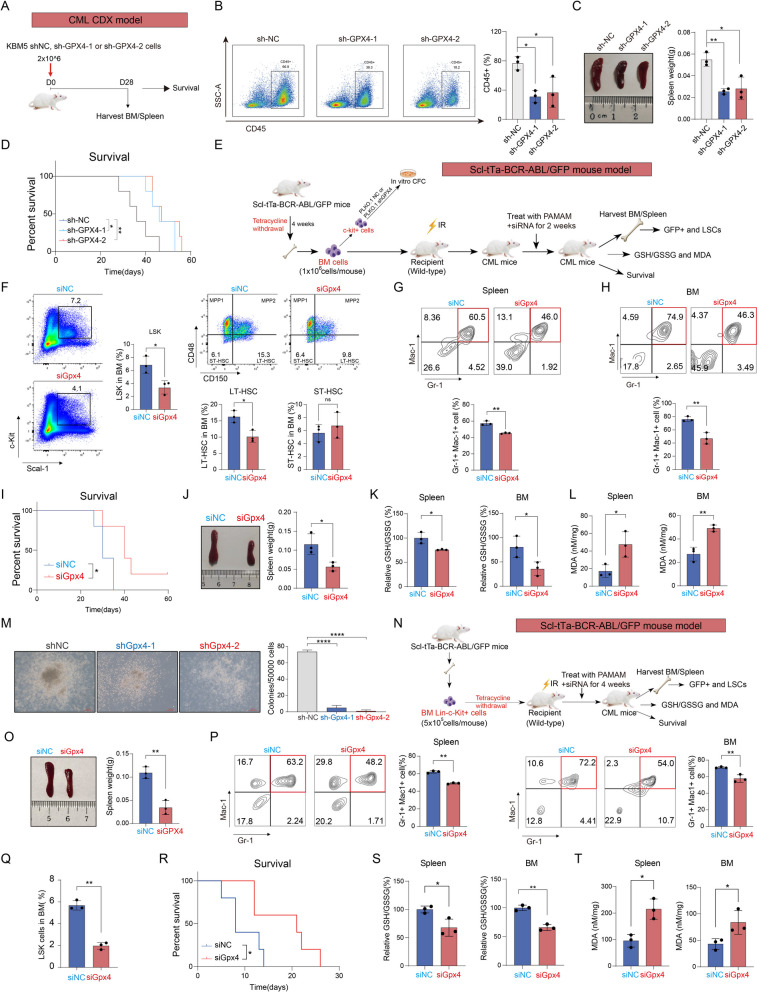
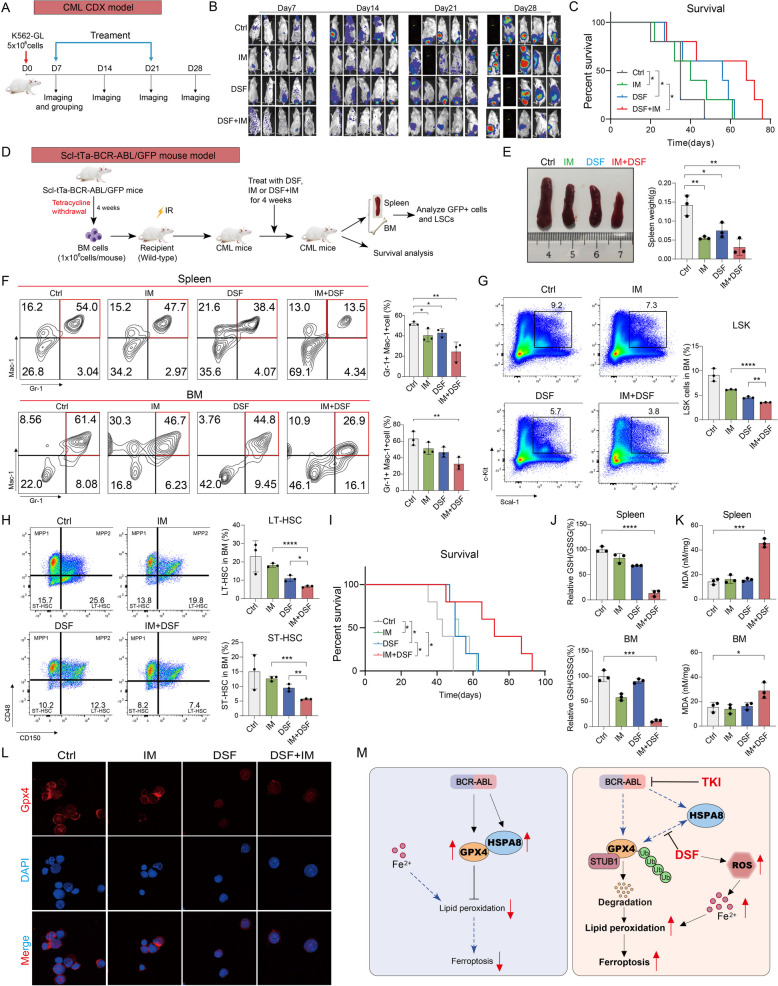
Results: Here, we present compelling evidence elucidating the sensitivity of DSF, an USA FDA-approved drug for alcohol dependence, towards BCR-ABL+ cells. Our findings underscore DSF's ability to selectively induce a potent cytotoxic effect on BCR-ABL+ cell lines and effectively inhibit primary BCR-ABL+ leukemia cells. Crucially, the combined treatment of DSF with TKIs selectively eradicates TKI-insensitive stem cells and resistant cells. Of particular note is DSF's capacity to disrupt GPX4 stability, elevate the labile iron pool, and intensify lipid peroxidation, ultimately leading to ferroptotic cell death. Our investigation shows that BCR-ABL expression induces alterations in cellular iron metabolism and increases GPX4 expression. Additionally, we demonstrate the indispensability of GPX4 for LSC development and the initiation/maintenance of BCR-ABL+ leukemia. Mechanical analysis further elucidates DSF's capacity to overcome resistance by reducing GPX4 levels through the disruption of its binding with HSPA8, thereby promoting STUB1-mediated GPX4 ubiquitination and subsequent proteasomal degradation. Furthermore, the combined treatment of DSF with TKIs effectively targets both BCR-ABL+ blast cells and drug-insensitive LSCs, conferring a significant survival advantage in mouse models.
Conclusion: In summary, the dual inhibition of GPX4 and BCR-ABL presents a promising therapeutic strategy to synergistically target blast cells and drug-insensitive LSCs in patients, offering potential avenues for advancing leukemia treatment.
Keywords: BCR-ABL+ leukemia; Disulfiram; Ferroptosis; GPX4; Tyrosine kinase inhibitor.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Liu C, et al. Loss of PRMT7 reprograms glycine metabolism to selectively eradicate leukemia stem cells in CML. Cell Metab. 2022;34(6):818-e8357. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
