

Risks of Organ Preservation in Rectal Cancer: Data From Two International Registries on Rectal Cancer
- PMID: 39467217
- PMCID: PMC12058371
- DOI: 10.1200/JCO.24.00405
Risks of Organ Preservation in Rectal Cancer: Data From Two International Registries on Rectal Cancer
Abstract
Purpose: Organ preservation has become an attractive alternative to surgery (total mesorectal excision [TME]) among patients with rectal cancer after neoadjuvant therapy who achieve a clinical complete response (cCR). Nearly 30% of these patients will develop local regrowth (LR). Although salvage resection is frequently feasible, there may be an increased risk for development of subsequent distant metastases (DM). The aim of this study is to compare the risk of DM between patients with LR after Watch and Wait (WW) and patients with near-complete pathologic response (nPCR) managed by TME at the time of reassessment of response.
Methods: Data from patients enrolled in the International Watch & Wait Database (IWWD) with cCR managed by WW and subsequent LR were compared with patients managed by TME (with ≤10% cancer cells-nPCR) from the Spanish Rectal Cancer Project (VIKINGO project). The primary end point was DM-free survival at 3 years from decision to WW or TME. The secondary end point was possible risk factors associated with DM.
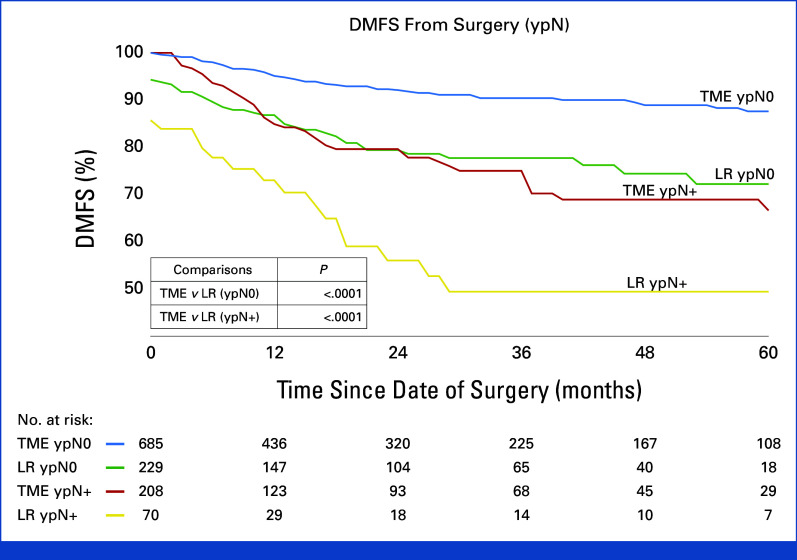
Results: Five hundred and eight patients with LR were compared with 893 patients with near-complete response after TME. Overall, DM rate was significantly higher among LRs (22.8% v 10.2%; P ≤ .001). Independent risk factors for DM included LR (v TME at reassessment; P = .001), ypT3-4 status (P = .016), and ypN+ status (P = .001) at the time of surgery. 3-year DM-free survival was significantly worse for patients with LR (75% v 87%; P = .001). When stratified for pathologic stage, patients with LR did significantly worse through all stages (P ≤ .009).
Conclusion: Patients with LR appear to have a higher risk for subsequent DM development than patients with nPCR managed by TME at restaging irrespective of final pathology. Leaving the primary undetectable tumor in situ until development of LR may result in worse oncologic outcomes.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures






References
-
- van der Valk MJM, Hilling DE, Bastiaannet E, et al. Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the international watch & wait database (IWWD): An International Multicentre Registry Study. Lancet. 2018;391:2537–2545. - PubMed
-
- Habr-Gama A, Sabbaga J, Gama-Rodrigues J, et al. Watch and wait approach following extended neoadjuvant chemoradiation for distal rectal cancer: Are we getting closer to anal cancer management? Dis Colon Rectum. 2013;56:1109–1117. - PubMed
-
- Chin RI, Roy A, Pedersen KS, et al. Clinical complete response in patients with rectal adenocarcinoma treated with short-course radiation therapy and nonoperative management. Int J Radiat Oncol Biol Phys. 2022;112:715–725. - PubMed
LinkOut - more resources
Full Text Sources
