

A clinical comparison of a digital versus conventional design methodology for transtibial prosthetic interfaces
- PMID: 39468101
- PMCID: PMC11519600
- DOI: 10.1038/s41598-024-74504-3
A clinical comparison of a digital versus conventional design methodology for transtibial prosthetic interfaces
Abstract
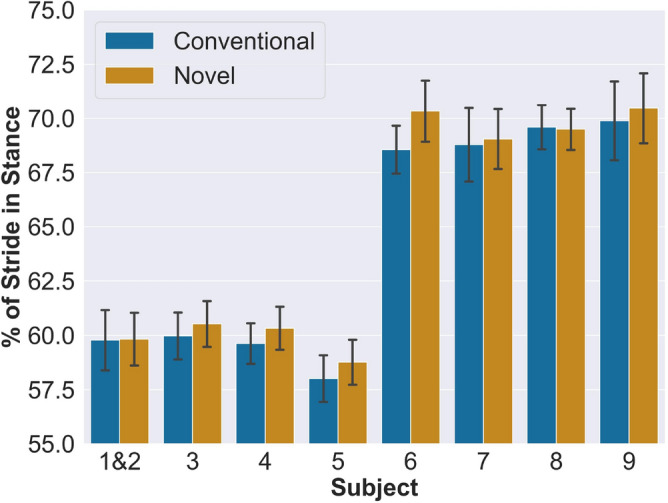
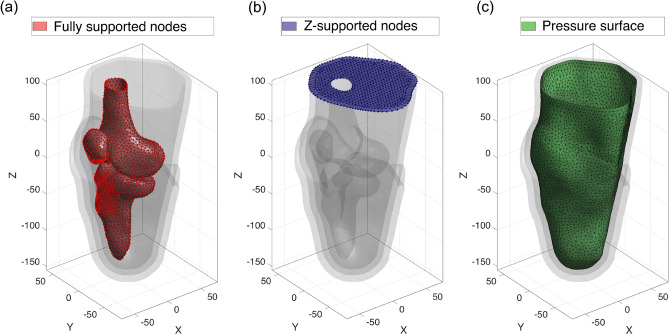
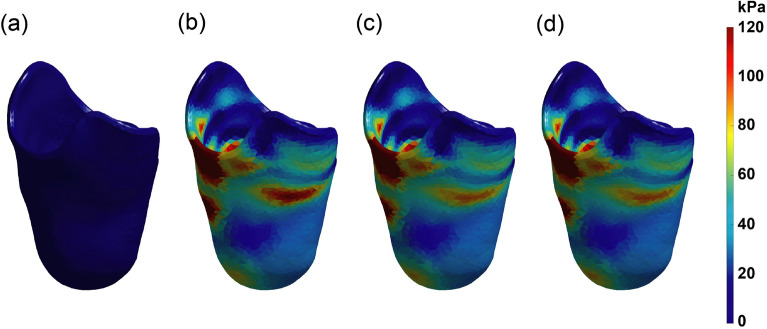
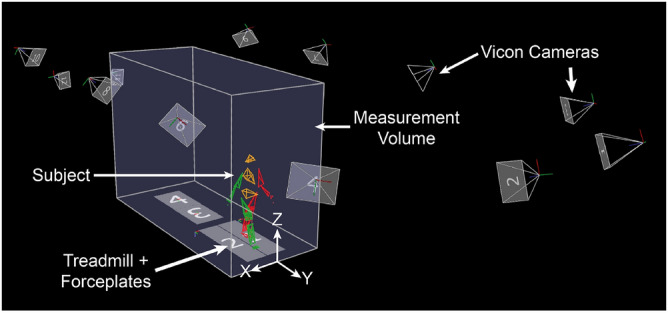
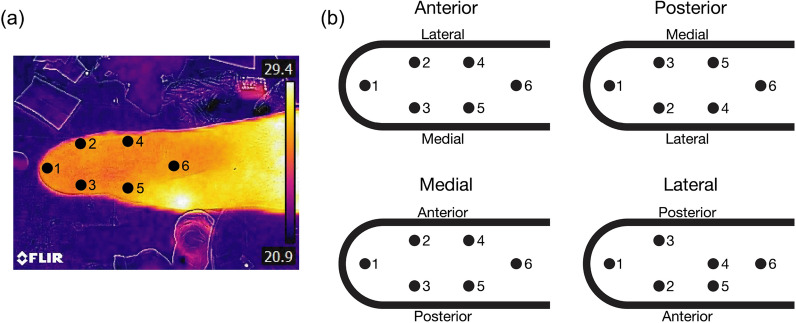
A transtibial prosthetic interface typically comprises a compliant liner and an outer rigid socket. The preponderance of today's conventional liners are mass produced in standard sizes, and conventional socket design is labor-intensive and artisanal, lacking clear scientific rationale. This work tests the clinical efficacy of a novel, physics-based digital design framework to create custom prosthetic liner-socket interfaces. In this investigation, we hypothesize that the novel digital approach will improve comfort outcomes compared to a conventional method of liner-socket design. The digital design framework generates custom transtibial prosthetic interfaces starting from MRI or CT image scans of the residual limb. The interface design employs FEA to simulate limb deformation under load. Interfaces are fabricated for 9 limbs from 8 amputees (1 bilateral). Testing compares novel and conventional interfaces across four assessments: 5-min walking trial, thermal imaging, 90-s standing pressure trial, and an evaluation questionnaire. Outcome measures include antalgic gait criterion, skin surface pressures, skin temperature changes, and direct questionnaire feedback. Antalgic gait is compared via a repeated measures linear mixed model while the other assessments are compared via a non-parametric Wilcoxon sign-rank test. A statistically significant ([Formula: see text]) decrease in pain is demonstrated when walking on the novel interfaces compared to the conventional. Standing pressure data show a significant decrease in pressure on novel interfaces at the anterior distal tibia ([Formula: see text]), with no significant difference at other measured locations. Thermal results show no statistically significant difference related to skin temperature. Questionnaire feedback shows improved comfort on novel interfaces on posterior and medial sides while standing and the medial side while walking. Study results support the hypothesis that the novel digital approach improves comfort outcomes compared to the evaluated conventional method. The digital interface design methodology also has the potential to provide benefits in design time, repeatability, and cost.
Keywords: 3D printing; Comfort; Custom; Digital design; FEA-based optimization; Prosthetics.
© 2024. The Author(s).
Conflict of interest statement
Authors Duncan R.C. Lee, Xingbang Yang, Dana Solav, Kevin M. Moerman, Christina I. Meyer, Aaron M. Jaeger, and Hugh M. Herr are listed as inventors on patent applications related to the presented transtibial liner-socket design methodology. All other authors do not have any competing interests.
Figures







References
-
- Murphy, E. F. Sockets, linings, and interfaces. Clin. Prosthet. Orthot.8, 4–10 (1984).
-
- Edwards, M. L. Lower limb prosthetics. In Clinician’s Guide to Assistive Technology 297–310. 10.1016/B978-081514601-8.50026-4 (Elsevier, 2002).
-
- McDonald, C. L., Westcott-McCoy, S., Weaver, M. R., Haagsma, J. & Kartin, D. Global prevalence of traumatic non-fatal limb amputation. Prosthet. Orthot. Int.45, 105–114. 10.1177/0309364620972258 (2021). - PubMed
-
- Highsmith, J. T. & Highsmith, M. J. Common skin pathology in LE prosthesis users. J. Am. Acad. Phys. Assist.20, 33–36. 10.1097/01720610-200711000-00018 (2007). - PubMed
-
- Spittle, M., Collins, R. J. & Conner, H. The incidence of pressure sores following lower limb amputations. Pract. Diabetes Int.18, 57–61. 10.1002/pdi.139 (2001).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
