

Established focal therapy-HIFU, IRE, or cryotherapy-where are we now?-a systematic review and meta-analysis
- PMID: 39468217
- PMCID: PMC12399424
- DOI: 10.1038/s41391-024-00911-2
Established focal therapy-HIFU, IRE, or cryotherapy-where are we now?-a systematic review and meta-analysis
Abstract
Introduction: Focal Therapy (FT) is a treatment option for the treatment of limited volume clinically significant prostate cancer (csPCa). We aim to systematically review outcomes of established FT modalities to assess the contemporary baseline and identify gaps in evidence that will aid in further trial and study design.
Methods: We conducted a systematic review and meta-analysis of all primary studies reporting outcomes of FT using cryotherapy, high-intensity focused ultrasound (HIFU), and irreversible electroporation (IRE). We described patient inclusion criteria, selection tools, treatment parameters, and surveillance protocols, and pooled overall survival (OS), cancer-specific survival (CSS), metastasis-free survival (MFS), biochemical progression (BP), biopsy, secondary treatment, sexual, and urinary function outcomes. Composite failure was defined as salvage whole gland ablation, radical treatment, hormonal therapy or transition to watchful waiting.
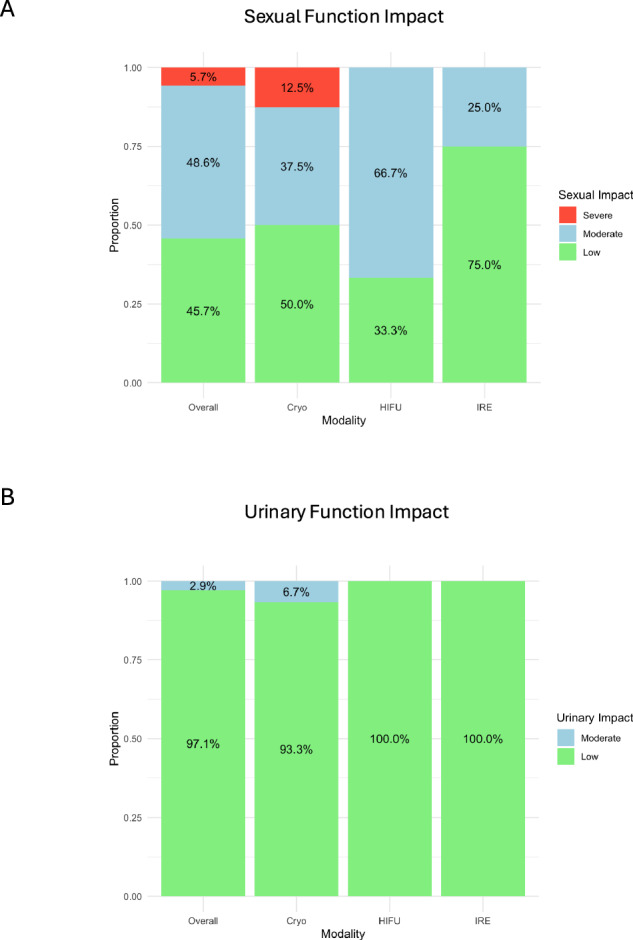
Synthesis: We identified 49 unique cohorts of men undergoing FT between 2008 and 2024 (21 cryotherapy, 20 HIFU, and 8 IRE). Median follow-up ranged from 6 to 63 months. Pooled OS was 98.0%, CSS 99.3%, and MFS 98.5%. Pooled BP was 9.4%/year. Biopsy was mandated post-FT within 24 months in 36/49 (73.5%) cohorts, with pooled csPCa (GG ≥ 2) rates of 22.2% overall, 8.9% infield, and 12.3% outfield. The pooled rate of secondary FT was 5.0%, radical treatment 10.5%, and composite failure 14.1%. Of 35 studies reporting sexual function, 45.7% reported a low, 48.6% moderate, and 5.7% severe impact. For 34 cohorts reporting urinary function, 97.1% reported a low impact. No differences were noted between cryotherapy, HIFU, or IRE in any of the outcomes.
Conclusion: FT with cryotherapy, HIFU, and IRE is associated with good short-intermediate term oncological and functional outcomes. However, outcome reporting is heterogeneous and often incomplete. Long-term follow-up and standardized reporting are required to better define and report FT outcomes.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: KJT reports personal fees and non-financial support from Boston Scientific; LRS and JLDE have consulted for AngioDynamics; OU has received non-financial support from Boston Scientific. AB has consulted for EDAP; The remaining authors have no conflicts to declare.
Figures




References
-
- Cornford P, van den Bergh RCN, Briers E, Van den Broeck T, Brunckhorst O, Darraugh J, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG guidelines on prostate cancer-2024 update. Part I: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2024;86:148–63. - PubMed
-
- Wallis CJ, Herschorn S, Saskin R, Su J, Klotz LH, Chang M, et al. Complications after radical prostatectomy or radiotherapy for prostate cancer: results of a population-based, propensity score-matched analysis. Urology. 2015;85:621–7. - PubMed
-
- Popiolek M, Rider JR, Andrén O, Andersson S-O, Holmberg L, Adami H-O, et al. Natural history of early, localized prostate cancer: a final report from three decades of follow-up. Eur Urol. 2013;63:428–35. - PubMed
-
- Klotz L, Vesprini D, Sethukavalan P, Jethava V, Zhang L, Jain S, et al. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol. 2015;33:272–7. - PubMed
-
- Tay KJ. Prostate focal therapy: the rule or exception? Curr Opin Urol. 2018;28:512–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
