

Early differences in lassitude predicts outcomes in Stanford Neuromodulation Therapy for difficult to treat depression
- PMID: 39468255
- PMCID: PMC11519532
- DOI: 10.1038/s44184-024-00099-2
Early differences in lassitude predicts outcomes in Stanford Neuromodulation Therapy for difficult to treat depression
Abstract
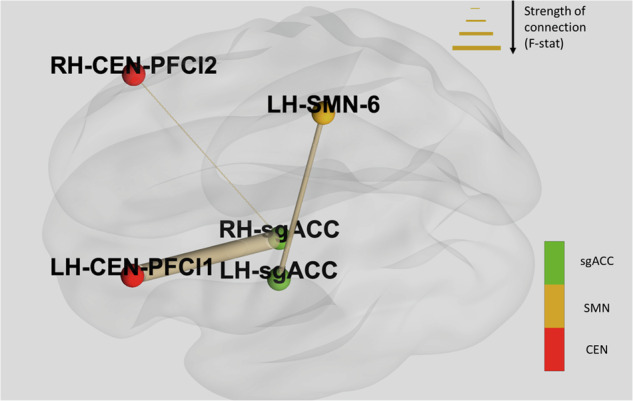
Stanford Neuromodulation Therapy (SNT), has recently shown rapid efficacy in difficult to treat (DTT) depression. We conducted an exploratory analysis of individual symptom improvements during treatment, correlated with fMRI, to investigate this rapid improvement in 23 DTT participants from an SNT RCT (12 active, 11 sham). Montgomery-Åsberg Depression Rating Scale item 7 (Lassitude) was the earliest to show improvements between active and sham, as early as treatment day 2. Lassitude score at treatment day 3 was predictive of response at 4 weeks post-treatment and response immediately after treatment. Participants with lower lassitude scores at treatment day 3 had different patterns of sgACC functional connectivity compared to participants with higher scores in both baseline and post-treatment minus baseline analyses. Further work will aim to first replicate these preliminary findings, and then to extend these findings and examine how SNT may affect lassitude and behavioral activation early in treatment.
© 2024. The Author(s).
Conflict of interest statement
N.R.W. is a named inventor on Stanford-owned intellectual property relating to accelerated TMS pulse pattern sequences and neuroimaging-based TMS targeting; he has served on scientific advisory boards for Otsuka, NeuraWell, Magnus Medical, and Nooma as a paid advisor; and he has equity/stock options in Magnus Medical, NeuraWell, and Nooma. D.B. is a founder, shareholder, and officer of Aifred Health, a digital mental health company whose work is unrelated to this article. All other investigators declare no conflicts of interest. D.B. is a founder and shareholder of CanadaNeuro, a mental health company whose work is unrelated to this publication and which did not support this work.
Figures


References
-
- Warden, D., Rush, A. J., Trivedi, M. H., Fava, M. & Wisniewski, S. R. The STAR*D project results: A comprehensive review of findings. Curr. Psychiatry Rep.9, 449–459 (2007). - PubMed
-
- Gaynes, B. N. et al. Repetitive transcranial magnetic stimulation for treatment-resistant depression. J. Clin. Psychiatry75, 477–489 (2014). - PubMed
-
- Fitzgerald, P. B. & Daskalakis, Z. J. Equipment and rTMS program setup. In rTMS Treatment for Depression 189–194 (Springer International Publishing, 2022).
LinkOut - more resources
Full Text Sources
