

Association Between Febuxostat Use and the Incidence of Cardiovascular Events, Mortality, and Kidney Events in Patients With Chronic Kidney Disease Compared to Allopurinol: A Study Using a Japanese Nationwide Database
- PMID: 39469391
- PMCID: PMC11513208
- DOI: 10.7759/cureus.70351
Association Between Febuxostat Use and the Incidence of Cardiovascular Events, Mortality, and Kidney Events in Patients With Chronic Kidney Disease Compared to Allopurinol: A Study Using a Japanese Nationwide Database
Abstract
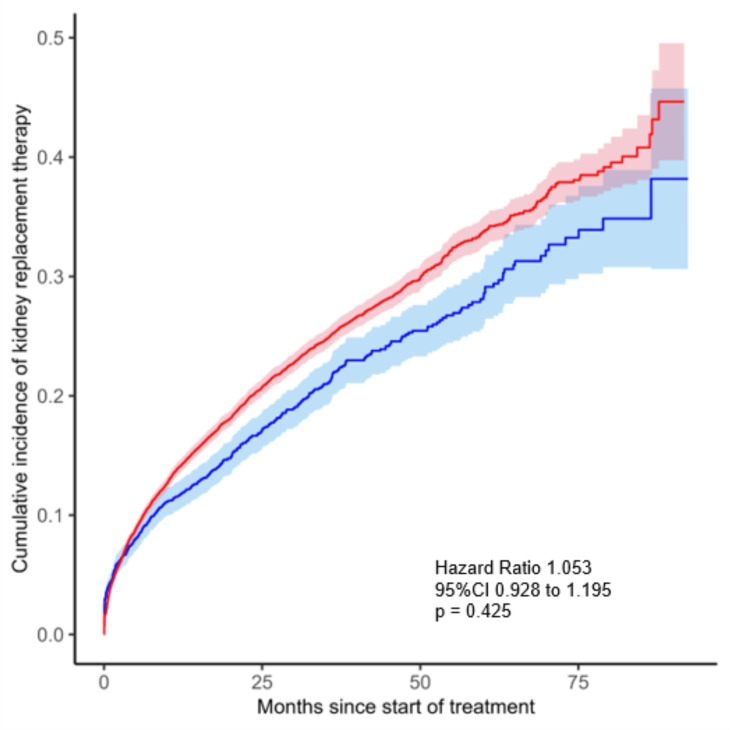
Background Patients with chronic kidney disease (CKD) were excluded in most trials that investigated the effects of urate-lowering agents, such as febuxostat and allopurinol, in hyperuricemic patients. This exclusion leads to uncertainty regarding the efficacy of febuxostat in patients with CKD. Due to the high prevalence of hyperuricemia in patients with CKD, we aimed to assess the effect of febuxostat on improving patient outcomes concerning cardiovascular events and survival compared with those treated with allopurinol among patients with CKD. Methods We conducted a retrospective cohort study using Japanese nationwide administrative data from Jan 1, 2013, to Sep 30, 2020. Patients aged over 60 years diagnosed with CKD were included in this study if they were prescribed either febuxostat or allopurinol. The primary outcome was the occurrence of cardiovascular events including myocardial infarction, stroke, unstable angina requiring urgent revascularization, and all-cause deaths. We estimated hazard ratios (HR) and 95% CI using a Cox proportional hazard regression model adjusted for comorbidities, medications, and laboratory data. We also assessed defined starting kidney replacement therapy as a secondary endpoint treating death as a competing risk using the Fine & Gray regression model. Results A total of 21,015 patients included those with febuxostat (n=17,796) and those with allopurinol (n=3,219). The association between the type of drug and the occurrence of cardiovascular events did not show a significant difference (0.107 vs. 0.116 events per patient-year; adjusted HR 0.953, 95% CI: 0.854 to 1.062, P=0.381). Similar results were seen for all-cause deaths (0.060 vs. 0.068 events per patient-year; adjusted HR 0.877, 95% CI: 0.760 to 1.012, P=0.073). Regarding the secondary endpoint, the association between the type of drug and the timing of starting kidney replacement therapy did not show a significant difference (0.118 vs. 0.097 events per patient-year; adjusted HR 0.953, 95% CI: 0.854 to 1.062, P=0.425). Conclusion The use of febuxostat was neither associated with a decreased risk of cardiovascular events or deaths nor with the timing of starting kidney replacement therapy compared to the use of allopurinol in patients with CKD.
Keywords: cardiovascular events; chronic kidney disease; database; hyperuricemia; kidney prognosis; kidney replacement therapy; mortality; renal prognosis; urate-lowering agent; uric acid.
Copyright © 2024, Otani et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: Ayumi Shintani is compensated by Kyowa Kirin, and the payment is made to the institution. Financial relationships: Ayumi Shintani declare(s) personal fees from Daiichi Sankyo. Payment was made to her. Ayumi Shintani declare(s) personal fees from Eisai. Payment was made to her. Ayumi Shintani declare(s) personal fees from Maruho. Payment was made to her. Ayumi Shintani declare(s) personal fees from Novo Nordisk Pharma. Payment was made to her. Ayumi Shintani declare(s) personal fees from Pfizer. Payment was made to her. Ayumi Shintani declare(s) personal fees from Taisho Pharmaceutical. Payment was made to her. Ayumi Shintani declare(s) personal fees from Torii Pharmaceutical. Payment was made to her. Ayumi Shintani declare(s) personal fees from Janssen Pharmaceutical. Payment was made to her. Ayumi Shintani declare(s) personal fees from Kisei Pharmaceutical. Payment was made to her. Ayumi Shintani declare(s) personal fees from Mallinckrodt Pharmaceuticals. Payment was made to her. Ayumi Shintani declare(s) personal fees from Mitsubishi Tanabe Pharma Corporation. Payment was made to her. Ayumi Shintani declare(s) personal fees from Nippon Shinyaku. Payment was made to her. Ayumi Shintani declare(s) personal fees from Ono Pharmaceutical Company Limited. Payment was made to her. Ayumi Shintani declare(s) personal fees from Takeda Pharmaceutical Company Limited. Payment was made to her. Ayumi Shintani declare(s) personal fees from Taisho Pharmaceutical. Payment was made to her. Ayumi Shintani declare(s) personal fees from Kyowa Kirin. Payment was made to her. Ayumi Shintani declare(s) personal fees from Merck Biopharma. Payment was made to her. Ayumi Shintani declare(s) personal fees from Nipro Corporation. Payment was made to her. Yuta Nonomiya declare(s) a grant from Osaka Metropolitan University. An annual fellowship of 3.9 million yen is paid to the author. Yasutaka Ihara declare(s) employment from Daiichi Sankyo. Yasutaka Ihara is an employee of Daiichi Sankyo. Kazuhiko Tsuruya declare(s) a grant from Teijin. Kazuhiko Tsuruya declare(s) a grant from Mochida. Kazuhiko Tsuruya declare(s) personal fees from Teijin. Kazuhiko Tsuruya declare(s) personal fees from Mochida. Kazuhiko Tsuruya declare(s) personal fees from Sanwa Chemical. Kazuhiko Tsuruya declare(s) personal fees from Fuji. Ayumi Shintani declare(s) personal fees from Chugai Pharmaceutical. Payment was made to the institution. Ayumi Shintani declare(s) personal fees from Daiichi Sankyo. Payment was made to the institution. Ayumi Shintani declare(s) personal fees from Kyowa Kirin. Payment was made to the institution and to her. Ayumi Shintani declare(s) personal fees from Takeda Pharmaceutical Company Limited. Payment was made to the institution. Ayumi Shintani declare(s) personal fees from Shionogi Pharma. Payment was made to her. Ayumi Shintani declare(s) personal fees from Abbvie. Payment was made to her. Ayumi Shintani declare(s) personal fees from Asahi Kasei Corporation. Payment was made to her. Ayumi Shintani declare(s) personal fees from AstraZeneca plc. Payment was made to her. Ayumi Shintani declare(s) personal fees from Astellas Pharma. Payment was made to her. Ayumi Shintani declare(s) personal fees from Bayer Yakuhin. Payment was made to her. Ayumi Shintani declare(s) personal fees from Bristol Myers Squibb. Payment was made to her. Ayumi Shintani declare(s) personal fees from Chugai Pharmaceutical. Payment was made to her. Ayumi Shintani declare(s) personal fees from Sanofi K.K. Payment was made to her. Ayumi Shintani declare(s) personal fees from Nippon Kayaku. Payment was made to her. Ayumi Shintani declare(s) personal fees from JCR Pharmaceuticals Co. Payment was made to her. Ayumi Shintani declare(s) personal fees from MSD. Payment was made to her. Hisako Yoshida declare(s) personal fees from Organization for Clinical Medicine Promotion. Other relationships: Febuxostat is sold by the following companies, which I declared in the COI: Teijin, DAIICHI SANKYO ESPHA CO., LTD., and NIPRO CORPORATION. Allopurinol is sold by the following companies, which I declared in the COI: NIPRO ES PHARMA and Shionogi Pharma Co. .
Figures








References
-
- Cardiovascular safety of febuxostat or allopurinol in patients with gout. White WB, Saag KG, Becker MA, et al. N Engl J Med. 2018;378:1200–1210. - PubMed
-
- Long-term cardiovascular safety of febuxostat compared with allopurinol in patients with gout (FAST): a multicentre, prospective, randomised, open-label, non-inferiority trial. Mackinzie IS, Ford I, Nuki G, et al. Lancet. 2020;28:1745–1757. - PubMed
LinkOut - more resources
Full Text Sources