

The biogeography of the mucosa-associated microbiome in health and disease
- PMID: 39469457
- PMCID: PMC11513579
- DOI: 10.3389/fmicb.2024.1454910
The biogeography of the mucosa-associated microbiome in health and disease
Abstract
Introduction: Little is known about the biogeography of the mucosa associated microbiome (MAM) in patients with inflammatory bowel disease (IBD) versus controls in different segments of the gastrointestinal tract, as well as the links between the MAM, gastrointestinal symptoms, and use of proton pump inhibitors (PPI).
Methods: We recruited 59 controls (without structural abnormalities and gastrointestinal symptoms), 44 patients with ulcerative colitis (UC) and 31 with Crohn's disease (CD). Biopsies from various segments of the upper and lower gastrointestinal tract were collected. Microbial composition was assessed via 16S rRNA gene amplicon analysis and the bacterial load of the mucosal biopsies were assessed via qPCR. The MAM was examined in the context of disease status, PPI usage, the severity of gastrointestinal symptoms, and the symptom response to a standardised nutrient challenge (SNC).
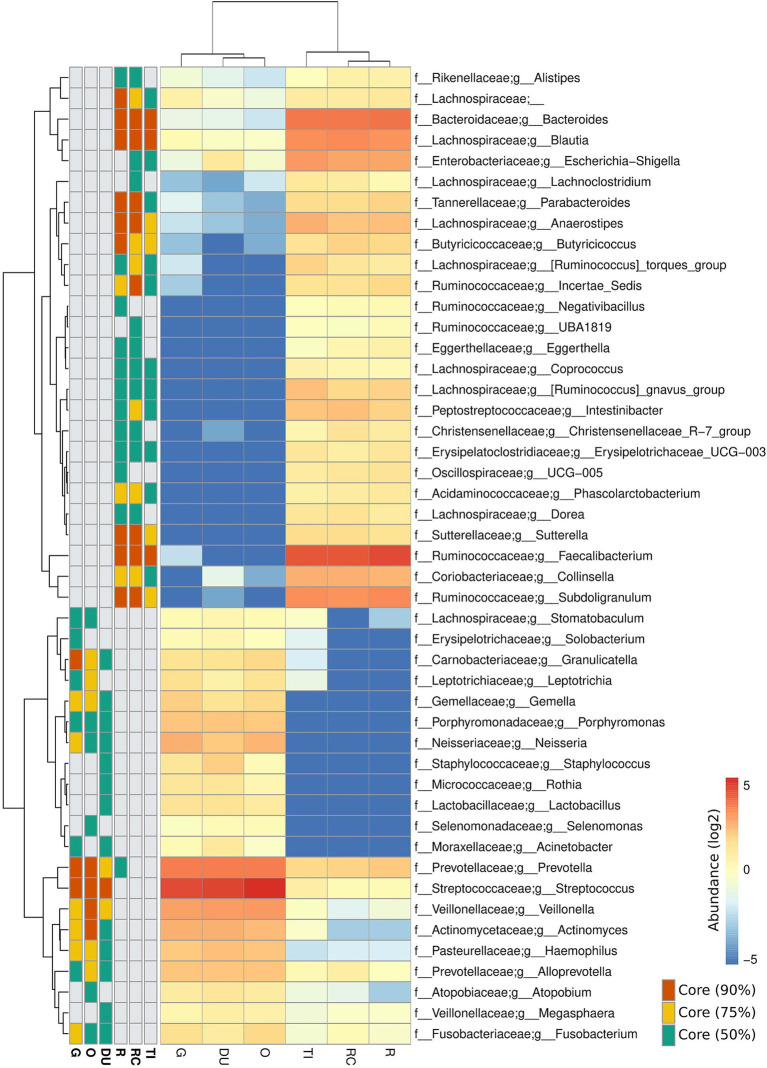
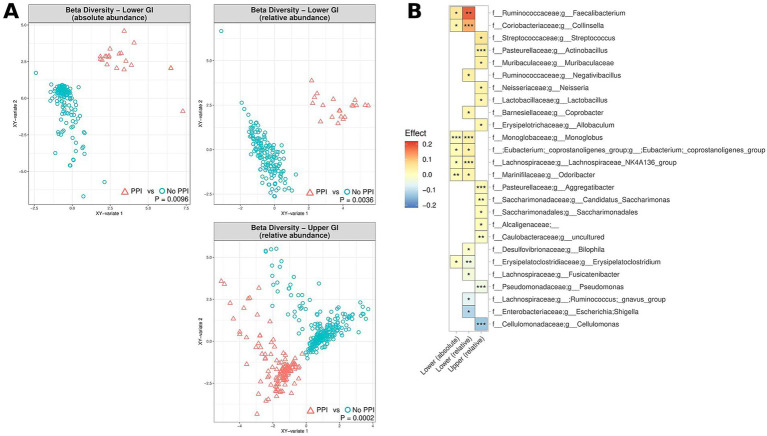
Results: Microbial communities of the MAM in the upper and lower gastrointestinal tract differed. IBD patients were characterised by relative and absolute depletion of numerous genera known to produce butyrate and/or propionate, with the largest differentiation being the depletion of Faecalibacterium in the lower gastrointestinal tract of CD patients. Notably, PPI users exhibited an enrichment of Faecalibacterium in the lower gastrointestinal tract. The severity of gastrointestinal symptoms, as well as the symptom response to the SNC, were significantly associated with MAM composition in the gastrointestinal tract.
Conclusion: The absolute and relative composition of the MAM is variable across different segments of the gastrointestinal tract. These quantitative changes indicates that MAM can be targeted in specific segments of the GI tract to improve patient outcomes.
Keywords: Crohn’s disease; gut-brain; microbiome; proton pump inhibitor; symptom severity; ulcerative colitis.
Copyright © 2024 Sternes, Shah, Ayala Pintos, Fairlie, Koloski, Kang, Tousignant, McIlroy, Morrison, Tyson and Holtmann.
Conflict of interest statement
GH reports to be on the advisory boards Australian Biotherapeutics, Glutagen, Bayer and received research support from Bayer, Abbott, Pfizer, Janssen, Takeda, Allergan. He serves on the Boards of the West Moreton Hospital and Health Service (WMHHS), Queensland, UQ Healthcare, Brisbane and the Gastro-Liga, Germany and is Chair of the WMHHS Board Quality and Safety Commitee. He has a patent for the Brisbane aseptic biopsy device and serves as Editor of the Gastro-Liga Newsletter. He is on the Research Committee of the Royal Australasian College of Physicians. GH acknowledges funding from the National Health and Medical Research Council (NHMRC) for the Centre for Research Excellence in Digestive Health. GH holds an MRFF and an NHMRC Ideas grant. MM has received research grants from Soho Flordis International (SFI) Australia Research, Bayer Steigerwald Arzneimittelwerk (Bayer Consumer Health) and Yakult-Nature Global Grant for Gut Health; speaker’s honoraria, and travel sponsorship from Janssen Australia; consultancy fees from Bayer Steigerwald Arzneimittelwerk (Bayer Consumer Health), Sanofi Australia, and Danone-Nutricia Australia; speaker honoraria and travel sponsorship from Perfect Company (China), and travel sponsorship from Yakult Inc. (Japan). MM is coinventor of PCT/AU2022/050556 “Diagnostic marker for functional gastrointestinal disorders” via the University of Newcastle and UniQuest (University of Queensland) and US20110076356 A1 “Novel Fibro-biotic bacterium isolate” via the US Department of Agriculture. MM also acknowledges funding from NHMRC Australia, Australian Research Council, Princess Alexandra Hospital Research Foundation, Medical Research Futures Fund of Australia, Helmsley Charitable Trust via the Australasian Gastrointestinal Research Foundation, and United States Department of Defense. MM serves on the science advisory board (non-remunerated) for GenieBiome, Hong Kong. GT is co-founder of Microba Life Sciences. Microba Life Sciences is a microbial genomics company developing microbiome-based diagnostics and therapeutics. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures




References
LinkOut - more resources
Full Text Sources