

A case of Cushing's syndrome in a pregnant woman associated with hypertension, hypokalemia, and gestational diabetes mellitus
- PMID: 39469560
- PMCID: PMC11512942
- DOI: 10.1007/s13340-024-00745-2
A case of Cushing's syndrome in a pregnant woman associated with hypertension, hypokalemia, and gestational diabetes mellitus
Abstract
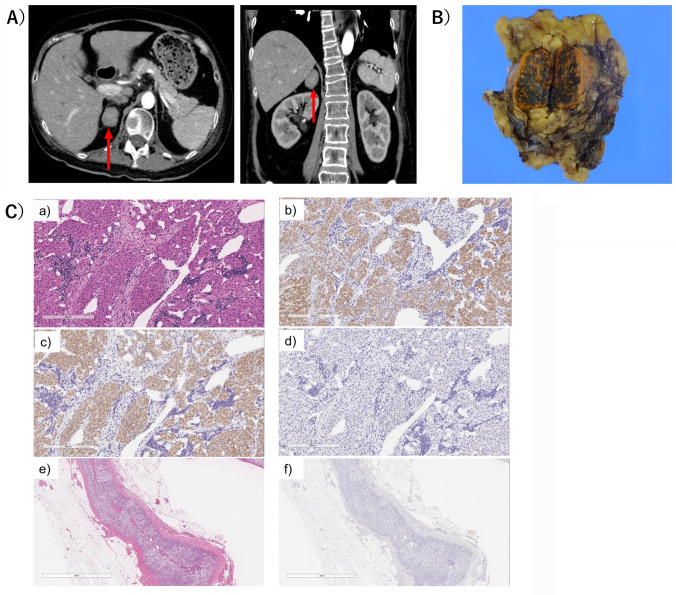
We report the case of a 33-year-old woman who was referred to the department of endocrinology and diagnosed with gestational diabetes mellitus (GDM). She had been hypertensive from 20 weeks of pregnancy. A 75 g oral glucose tolerance test for screening of GDM at 26 weeks of pregnancy revealed positive results at two points: 183 mg/dL at 60 min, and 193 mg/dL at 90 min. At the first visit to the Department of Endocrinology, Cushing's features were clinically unclear. She started self-monitoring blood glucose levels, and hypokalemia was detected. At 28 weeks of pregnancy, she was admitted to our hospital because of uncontrolled blood pressure. The patient started multiple injections of rapid insulin for postprandial hyperglycemia. Laboratory testing revealed suppressed plasma ACTH (< 1.5 pg/mL) and elevated serum cortisol levels (34.1 μg/dL) in the early morning. Because of uncontrollable pregnancy related complications, the patient delivered a baby by Caesarean section at 29 weeks of pregnancy. After delivery, she was diagnosed with ACTH-independent Cushing's syndrome by endocrinological tests. Computed tomography scan demonstrated a right adrenal tumor measuring 24 mm at greatest dimension. Twenty-three days after delivery, laparoscopic right adrenalectomy was performed. The diagnosis of cortisol-producing adrenocortical adenoma was pathologically confirmed. After surgery, the patient was given glucocorticoids as a replacement, and her blood pressure, blood glucose, and serum potassium levels were normalized. Although rare, GDM may be caused by Cushing's syndrome. Pregnant women with combinations of GDM, hypertension, and hypokalemia should be clinically suspected as harboring Cushing's syndrome even in the absence of specific clinical features.
Keywords: Adrenocortical adenoma; Cushing’s syndrome; Gestational diabetes mellitus; Gestational hypertension; Pregnancy.
© The Japan Diabetes Society 2024. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Conflict of interest statement
Ethical approvalThe authors have no potential conflicts of interest to disclose. This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures
References
-
- Caimari F, Valassi E, Garbayo P, Steffensen C, Santos A, Corcoy R, et al. Cushing’s syndrome and pregnancy outcomes: a systematic review of published cases. Endocrine. 2017;55:555–63. - PubMed
-
- HAPO Study Cooperative Research Group, Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008;358(19):1991–2002. - PubMed
-
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel, Metzger BE, Gabbe SG, Persson B, Buchanan TA, Catalano PA, Damm P, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676–82. - PMC - PubMed
-
- Weiss LM. Comparative histologic study of 43 metastasizing and nonmetastasizing adrenocortical tumors. Am J Surg Pathol. 1984;8:163–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources