

Characterizing Nonculprit Lesions and Perivascular Adipose Tissue of Patients Following Acute Myocardial Infarction Using Coronary Computed Tomography Angiography: A Comparative Study
- PMID: 39470055
- PMCID: PMC11935734
- DOI: 10.1161/JAHA.124.037258
Characterizing Nonculprit Lesions and Perivascular Adipose Tissue of Patients Following Acute Myocardial Infarction Using Coronary Computed Tomography Angiography: A Comparative Study
Abstract
Background: The comparison of coronary computed tomography angiography plaques and perivascular adipose tissue (PVAT) between patients with acute myocardial infarction (AMI) posttreatment and patients with stable coronary artery disease is poorly understood. Our objective was to evaluate the differences in coronary computed tomography angiography-quantified plaque and PVAT characteristics in patients post-AMI and identify signs of residual inflammation.
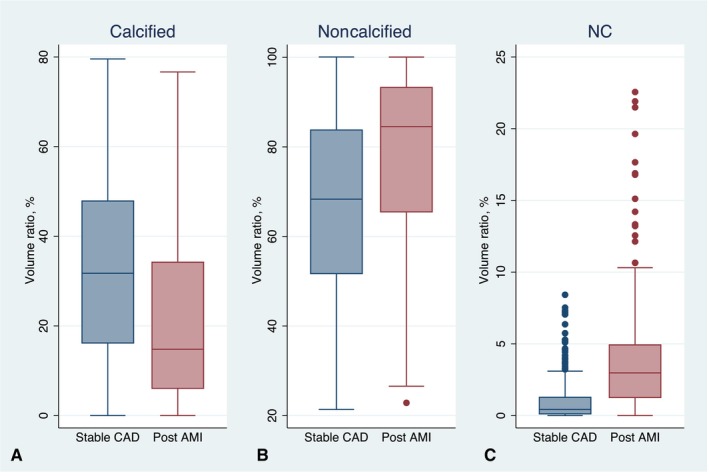
Methods and results: We analyzed 205 patients (age, 59.77±9.24 years; 92.20% men) with AMI ≤1 month and matched them with 205 patients with stable coronary artery disease (age, 60.52±10.04 years; 90.24% men) based on age, sex, and cardiovascular risk factors. Coronary computed tomography angiography scans were assessed for nonculprit plaque and vessel characteristics, plaque volumes by composition, high-risk plaques, and PVAT mean attenuation. Both patient groups exhibited similar noncalcified plaque volumes (383.35±313.23 versus 378.63±426.25 mm3, P=0.899). However, multivariable analysis revealed that patients post-AMI had a greater patient-wise noncalcified plaque volume ratio (estimate, 0.089 [95% CI, 0.053-0.125], P<0.001), largely attributed to a higher fibrofatty and necrotic core volume ratio, along with higher peri-lesion PVAT mean attenuation (estimate, 3.968 [95% CI, 2.556-5.379], P<0.001). When adjusted for vessel length, patients post-AMI had more high-risk plaques (estimate, 0.417 [95% CI, 0.298-0.536], P<0.001) per patient.
Conclusions: Patients post-AMI displayed heightened noncalcified plaque components, largely due to fibrofatty and necrotic core content, more high-risk plaques, and increased PVAT mean attenuation on a per-patient level, highlighting the necessity for refined risk assessment in patients with AMI after treatment.
Keywords: acute myocardial infarction; coronary atheroma; coronary computed tomography angiography; high‐risk plaques; residual inflammatory risk.
Figures






References
-
- Motoyama S, Ito H, Sarai M, Kondo T, Kawai H, Nagahara Y, Harigaya H, Kan S, Anno H, Takahashi H, et al. Plaque characterization by coronary computed tomography angiography and the likelihood of acute coronary events in mid‐term follow‐up. J Am Coll Cardiol. 2015;66:337–346. doi: 10.1016/j.jacc.2015.05.069 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
