

Neuroimaging to Genotype: Delineating the Spectrum of Disorders With Deficient Myelination in the Indian Population
- PMID: 39470296
- PMCID: PMC7617591
- DOI: 10.1002/ajmg.a.63914
Neuroimaging to Genotype: Delineating the Spectrum of Disorders With Deficient Myelination in the Indian Population
Abstract
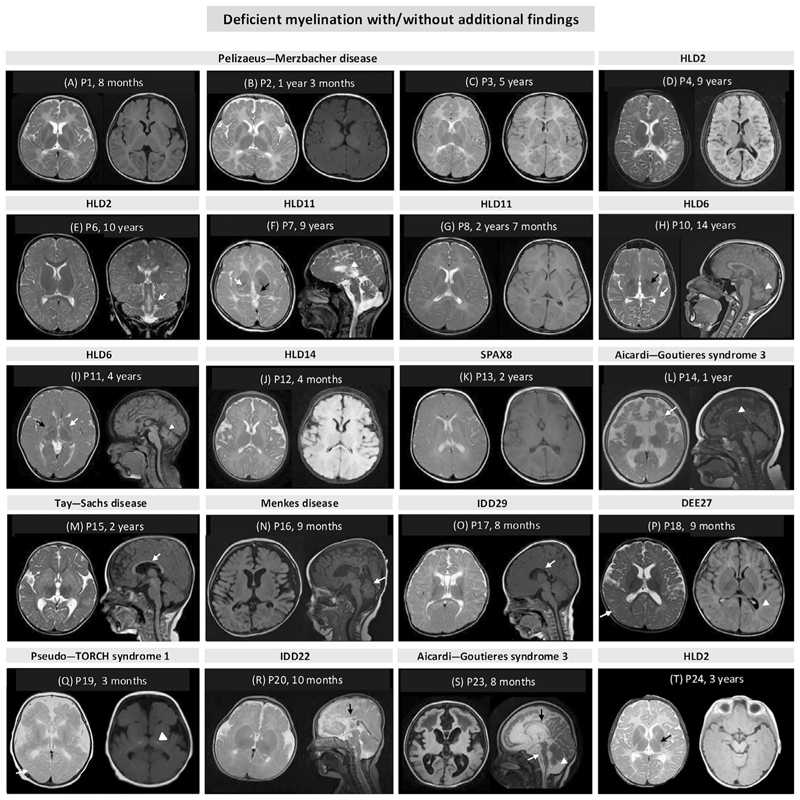
Several genetic disorders are associated with either a permanent deficit or a delay in central nervous system myelination. We investigated 24 unrelated families (25 individuals) with deficient myelination after clinical and radiological evaluation. A combinatorial approach of targeting and/or genomic testing was employed. Molecular diagnosis was achieved in 22 out of 24 families (92%). Four families (4/9, 44%) were diagnosed with targeted testing and 18 families (18/23, 78%) were diagnosed using broad genomic testing. Overall, 14 monogenic disorders were identified. Twenty disease-causing variants were identified in 14 genes including PLP1, GJC2, POLR1C, TUBB4A, UFM1, NKX6-2, DEGS1, RNASEH2C, HEXA, ATP7A, SETBP1, GRIN2B, OCLN, and ZBTB18. Among these, nine (45%) variants are novel. Fourteen families (82%, 14/17) were diagnosed using proband-only exome sequencing (ES) complemented with deep phenotyping, thus highlighting the utility of singleton ES as a valuable diagnostic tool for identifying these disorders in resource-limited settings.
Keywords: deficient myelination; genomics; myelin; neuroimaging.
© 2024 Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Arai-Ichinoi N, Uematsu M, Sato R, et al. Genetic Heterogeneity in 26 Infants With a Hypomyelinating Leukodystrophy. Human Genetics. 2016;135(1):89–98. - PubMed
-
- Bae H-G, Kim TK, Suk HY, Jung S, Jo D-G. White Matter and Neurological Disorders. Archives of Pharmacal Research. 2020;43(9):920–931. - PubMed
-
- Barkovich AJ, Deon S. Hypomyelinating Disorders: An MRI Approach. Neurobiology of Disease. 2016;87:50–58. - PubMed
-
- Brandt T, Sack LM, Arjona D, et al. Adapting ACMG/AMP Sequence Variant Classification Guidelines for Single-Gene Copy Number Variants. Genetics in Medicine. 2020;22(2):336–344. - PubMed
-
- Branson HM. Normal Myelination. Neuroimaging Clinics of North America. 2013;23(2):183–195. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
