

Outcomes of patients with acute liver failure not listed for liver transplantation: A cohort analysis
- PMID: 39470433
- PMCID: PMC11524736
- DOI: 10.1097/HC9.0000000000000575
Outcomes of patients with acute liver failure not listed for liver transplantation: A cohort analysis
Abstract
Background: Acute liver failure (ALF) is a rare condition leading to morbidity and mortality. Liver transplantation (LT) is often required, but patients are not always listed for LT. There is a lack of data regarding outcomes in these patients. Our aim is to describe outcomes of patients with ALF not listed for LT and to compare this with those listed for LT.
Methods: Retrospective analysis of all nonlisted patients with ALF enrolled in the Acute Liver Failure Study Group (ALFSG) registry between 1998 and 2018. The primary outcome was 21-day mortality. Multivariable logistic regression was done to identify factors associated with 21-day mortality. The comparison was then made with patients with ALF listed for LT.
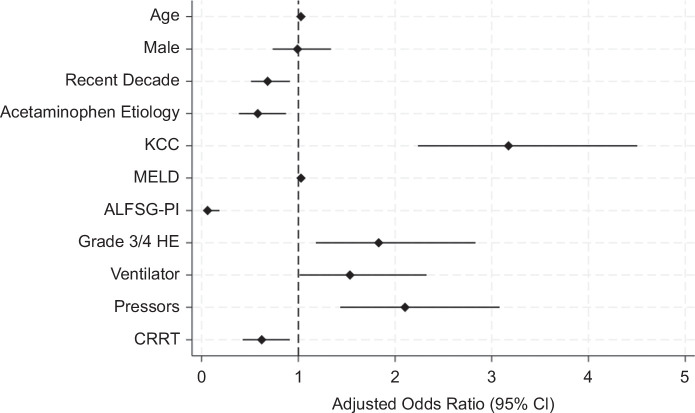
Results: A total of 1672 patients with ALF were not listed for LT. The median age was 41 (IQR: 30-54). Three hundred seventy-one (28.9%) patients were too sick to list. The most common etiology was acetaminophen toxicity (54.8%). Five hundred fifty-eight (35.7%) patients died at 21 days. After adjusting for relevant covariates, King's College Criteria (adjusted odds ratio: 3.17, CI 2.23-4.51), mechanical ventilation (adjusted odds ratio: 1.53, CI: 1.01-2.33), and vasopressors (adjusted odds ratio: 2.10, CI: 1.43-3.08) (p < 0.05 for all) were independently associated with 21-day mortality. Compared to listed patients, nonlisted patients had higher mortality (35.7% vs. 24.3%). Patients deemed not sick enough had greater than 95% survival, while those deemed too sick still had >30% survival.
Conclusions: Despite no LT, the majority of patients were alive at 21 days. Survival was lower in nonlisted patients. Clinicians are more accurate in deeming patients not sick enough to require LT as opposed to deeming patients too sick to survive.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Association for the Study of Liver Diseases.
Conflict of interest statement
William M. Lee receives research support from Merck, Conatus, Intercept, Bristol-Myers Squibb, Novo Nordisk, Synlogic, Eiger, Cumberland, Exalenz, Instrumentation Laboratory, and Ocera Therapeutics, now Mallinckrodt Pharmaceuticals, and has received personal fees for consulting from Forma, Sanofi, Seattle Genetics, Affibody, Karuna, and Genentech. The remaining authors have no conflicts to report.
Figures
References
-
- Bernal W, Auzinger G, Dhawan A, Wendon J. Acute liver failure. Lancet. 2010;376:190–201. - PubMed
-
- Dong V, Nanchal R, Karvellas CJ. Pathophysiology of acute liver failure. Nutr Clin Pract. 2020;35:24–29. - PubMed
-
- Williams R, Schalm SW, O'Grady JG. Acute liver failure: Redefining the syndromes. Lancet. 1993;342:273–275. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
