

US Clinical Practice Experience with Eculizumab in Myasthenia Gravis: Acute Clinical Events and Healthcare Resource Utilization
- PMID: 39470958
- PMCID: PMC11589080
- DOI: 10.1007/s40801-024-00457-8
US Clinical Practice Experience with Eculizumab in Myasthenia Gravis: Acute Clinical Events and Healthcare Resource Utilization
Abstract
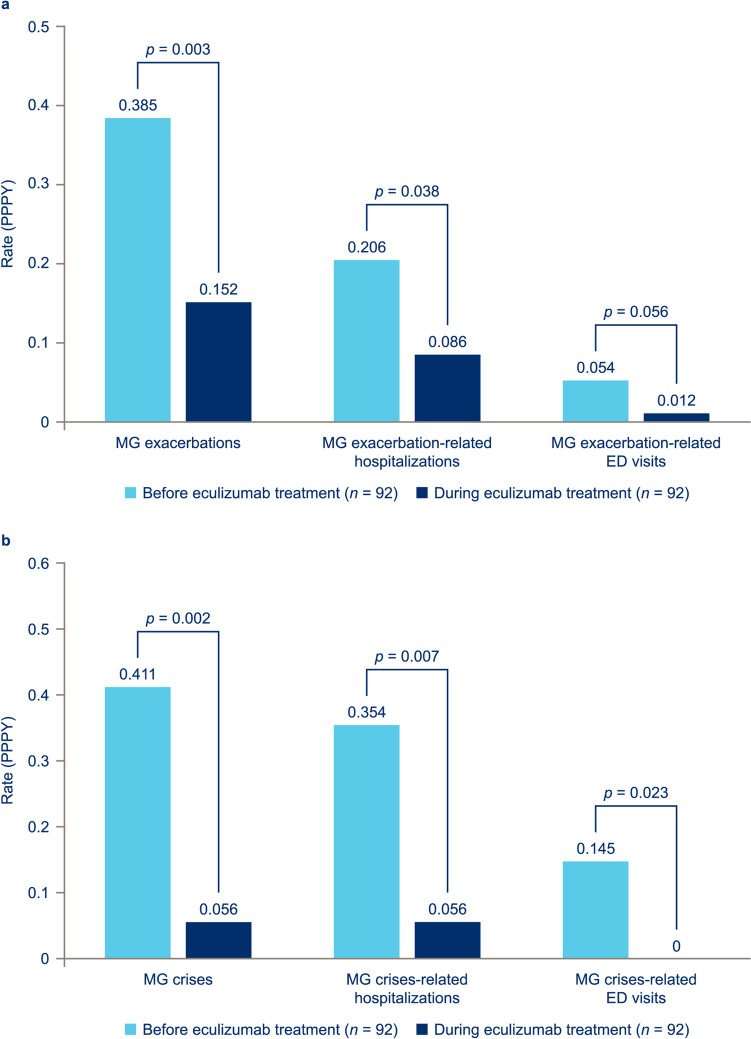
Background and objective: The terminal complement inhibitor eculizumab is approved in the USA for the treatment of patients with acetylcholine receptor antibody-positive generalized myasthenia gravis (MG). The ELEVATE study aimed to examine clinical-practice outcome data on eculizumab effectiveness in US adults with MG (generalized or ocular). This paper reports the findings on MG exacerbations and crises and associated healthcare resource utilization, and the use of rescue therapy.
Methods: A retrospective chart review was conducted of US adults with MG who initiated eculizumab. Outcomes assessed for up to 2 years before and after eculizumab initiation included percentages and rates per patient per year (PPPY) of exacerbations and crises (the latter defined as intubation/impending intubation), healthcare resource utilization, and rescue therapy administration.
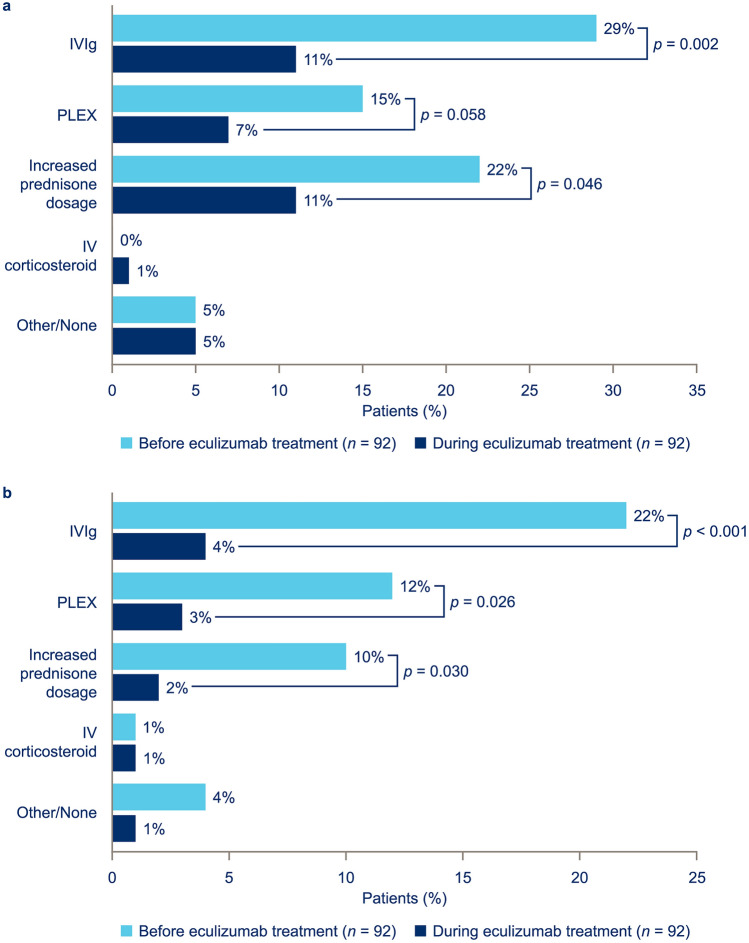
Results: A total of 119 patients diagnosed with MG were enrolled in the study; 92 patients had ≥ 3 months of data both before and during eculizumab therapy and were included in the analyses. The mean rate of MG exacerbations decreased from 0.385 PPPY before eculizumab initiation to 0.152 PPPY during eculizumab treatment (p = 0.0034); the mean rate of MG crises decreased from 0.411 to 0.056 PPPY (p = 0.0018). Rates of healthcare resource utilization and rescue therapy use also decreased significantly during eculizumab treatment.
Conclusions: This retrospective chart review analysis provides evidence for a beneficial impact of eculizumab treatment on the incidence of MG exacerbations and crises and associated healthcare resource utilization in clinical practice, and on rescue therapy use. These data further support the therapeutic benefits of eculizumab in patients with MG.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Funding: Research funding for this study and funding for medical writing assistance and open-access fees were provided by Alexion, AstraZeneca Rare Disease. Conflict of interest: Richard J. Nowak has received research support from Alexion, AstraZeneca Rare Disease, argenx, Genentech, Grifols, Immunovant, Inc., Momenta Pharmaceuticals, the Myasthenia Gravis Foundation of America, the National Institutes of Health (National Institute of Neurological Disorders and Stroke and National Institute of Allergy and Infectious Diseases), Ra Pharmaceuticals (now UCB), and Viela Bio Inc. (now Horizon Therapeutics); and consultancy fees from Alexion, AstraZeneca Rare Disease, argenx, Cour Pharmaceuticals, Grifols, Immunovant, Inc., Momenta Pharmaceuticals, Ra Pharmaceuticals (now UCB), Roivant Sciences, and Viela Bio (now Horizon Therapeutics). Ali A. Habib has served as a medical advisor and speaker on behalf of Alexion and AstraZeneca Rare Disease; he has received research support from Alexion, AstraZeneca Rare Disease, and Cabaletta Bio; and has received research support and honoraria from argenx, UCB, Pfizer, Genentech, Viela Bio, and Regeneron. Andrew J. Klink is a salaried employee of and owns stock in Cardinal Health, which received funding from Alexion, AstraZeneca Rare Disease for work performed on this study. Srikanth Muppidi has served on advisory board meetings for Alexion, AstraZeneca Rare Disease, argenx, Horizon Therapeutics, and Ra Pharmaceuticals (now UCB). Anju Parthan was an employee of Alexion, AstraZeneca Rare Disease, and owned stock in AstraZeneca at the time the study was conducted and analyzed. S. Chloe Sader is an employee of Alexion, AstraZeneca Rare Disease and owns stock in AstraZeneca. Alexandrina Balanean is a salaried employee of Cardinal Health, which received funding from Alexion, AstraZeneca Rare Disease for work performed on this study. Ajeet Gajra was a salaried employee of and owned stock in Cardinal Health, which received funding from Alexion, AstraZeneca Rare Disease for work performed on this study, at the time the study was conducted. James F. Howard Jr has received research support (paid to institution) from Ad Scientiam, Alexion, AstraZeneca Rare Disease, argenx, Cartesian Therapeutics, the Centers for Disease Control and Prevention (Atlanta, GA, USA), the Myasthenia Gravis Foundation of America, the Muscular Dystrophy Association, the National Institutes of Health (including the National Institute of Neurological Disorders and Stroke and the National Institute of Arthritis and Musculoskeletal and Skin Diseases), PCORI, and UCB Pharma; honoraria from Alexion AstraZeneca Rare Disease, Amgen, argenx, Biohaven Ltd, Biologix Pharma, CheckRare CME, F. Hoffman-LaRoche, Medscape CME, Merck EMD Serono, NMD Pharma, Novartis Pharma, PeerView CME, Physicians’ Education Resource CME, PlatformQ CME, Regeneron Pharmaceuticals, Sanofi US, UCB Pharma, and Zai Lab; and non-financial support from Alexion, AstraZeneca Rare Disease, argenx, Biohaven Ltd, Toleranzia AB, UCB Pharma, and Zai Lab. Ethics approval: The study was reviewed by the Western Institutional Review Board and determined exempt from requiring ethical approval on the basis that the study collected only secondary data, which were limited and comprised only necessary protected health information (e.g., treatment dates, date of death), and that all data were de-identified and aggregated. Consent to participate: As this study involves anonymized structured data, which according to applicable legal requirements do not contain data subject to privacy laws, obtaining informed consent from patients was not required. Consent for publication: Not applicable. Availability of data and material: Alexion, AstraZeneca Rare Disease will consider requests for disclosure of clinical study participant-level data provided that participant privacy is assured through methods such as data de-identification, pseudonymization, or anonymization (as required by applicable law), and if such disclosure was included in the relevant study an informed consent form or similar documentation. Qualified academic investigators may request participant-level clinical data and supporting documents (statistical analysis plan and protocol) pertaining to Alexion-sponsored studies. Further details regarding data availability and instructions for requesting information are available in the Alexion Clinical Trials Disclosure and Transparency Policy at https://www.alexionclinicaltrialtransparency.com/data-requests/ . Code availability: Not applicable. Author contributions: Study concept: RJN, AJK, SM, AP, SCS, AG. Study design: RJN, AJK, SM, AP, SCS, AB, AG, JFH Jr. Data acquisition: AAH, JFH Jr. Data analysis: RJN, AJK, AP, SCS, AB, AG. Data interpretation: all authors. Drafting/revision of the article for content: all authors. All authors read and approved the final version.
Figures
References
-
- Silvestri NJ, Wolfe GI. Treatment-refractory myasthenia gravis. J Clin Neuromuscul Dis. 2014;15(4):167–78. 10.1097/CND.0000000000000034. - PubMed
-
- Engel-Nitz NM, Boscoe A, Wolbeck R, Johnson J, Silvestri NJ. Burden of illness in patients with treatment refractory myasthenia gravis. Muscle Nerve. 2018;58(1):99–105. 10.1002/mus.26114. - PubMed
-
- Gummi RR, Kukulka NA, Deroche CB, Govindarajan R. Factors associated with acute exacerbations of myasthenia gravis. Muscle Nerve. 2019;60(6):693–9. 10.1002/mus.26689. - PubMed
