

Prospective phase II trial of [68Ga]Ga-NOTA-AE105 uPAR-PET/MRI in patients with primary gliomas: Prognostic value and Implications for uPAR-targeted Radionuclide Therapy
- PMID: 39472354
- PMCID: PMC11522270
- DOI: 10.1186/s13550-024-01164-9
Prospective phase II trial of [68Ga]Ga-NOTA-AE105 uPAR-PET/MRI in patients with primary gliomas: Prognostic value and Implications for uPAR-targeted Radionuclide Therapy
Abstract
Background: Treatment of patients with low-grade and high-grade gliomas is highly variable due to the large difference in survival expectancy. New non-invasive tools are needed for risk stratification prior to treatment. The urokinase plasminogen activator receptor (uPAR) is expressed in several cancers, associated with poor prognosis and may be non-invasively imaged using uPAR-PET. We aimed to investigate the uptake of the uPAR-PET tracer [68Ga]Ga-NOTA-AE105 in primary gliomas and establish its prognostic value regarding overall survival (OS), and progression-free survival (PFS). Additionally, we analyzed the proportion of uPAR-PET positive tumors to estimate the potential number of candidates for future uPAR-PRRT.
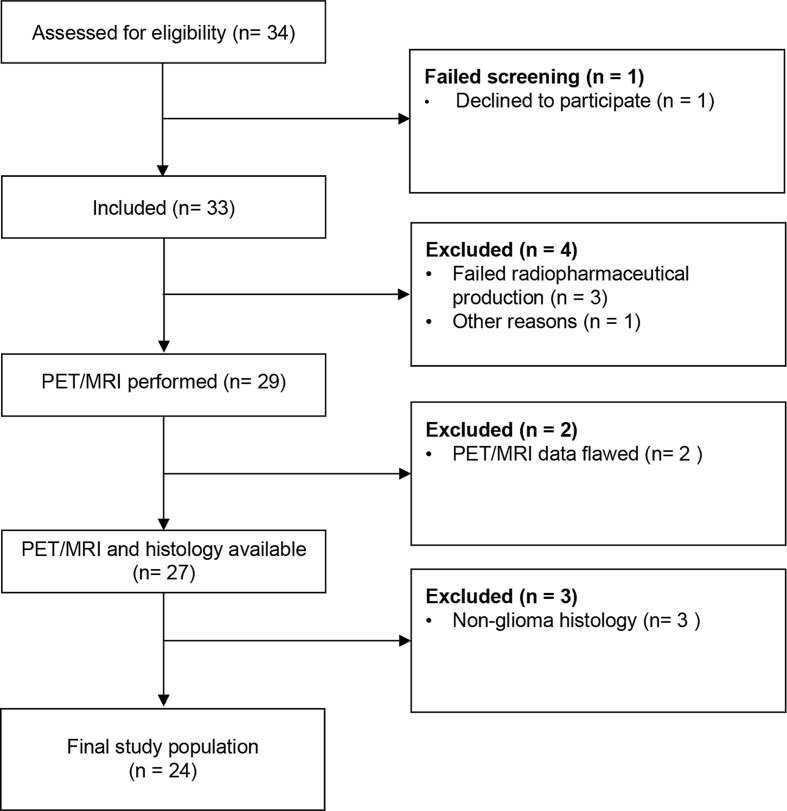
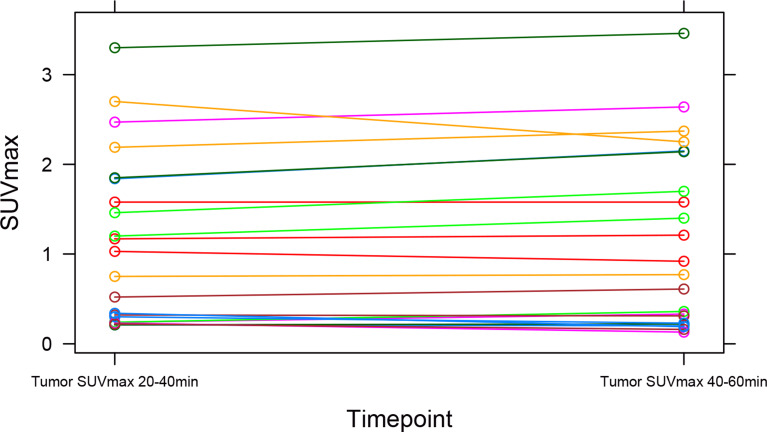
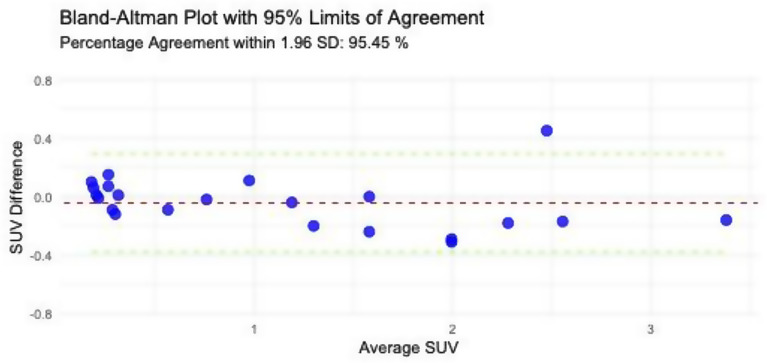
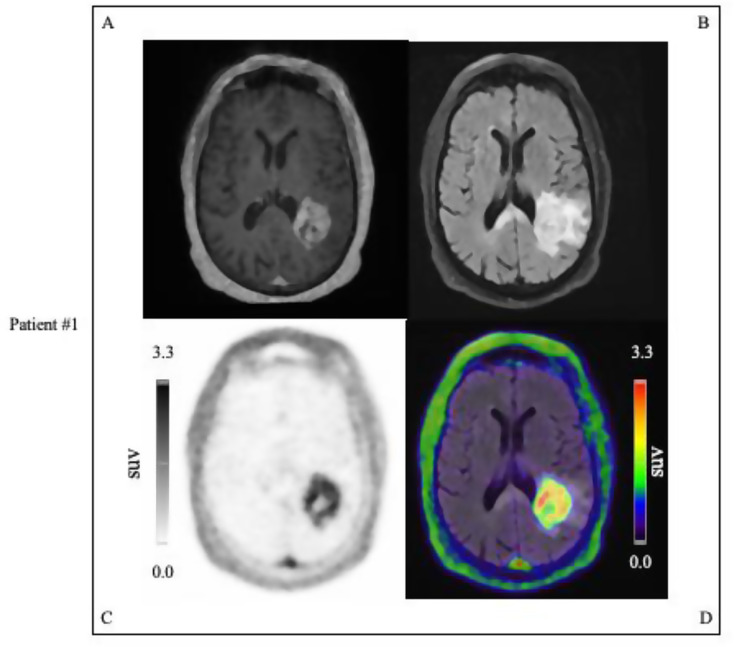
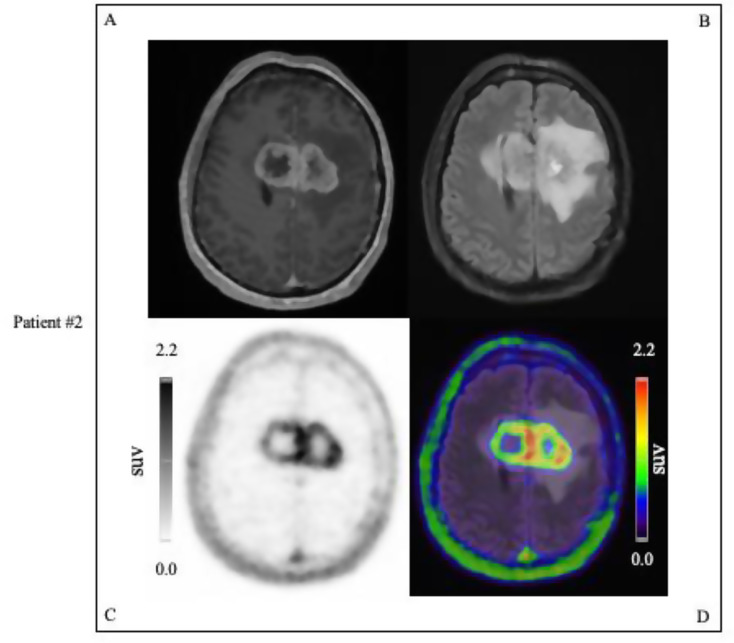
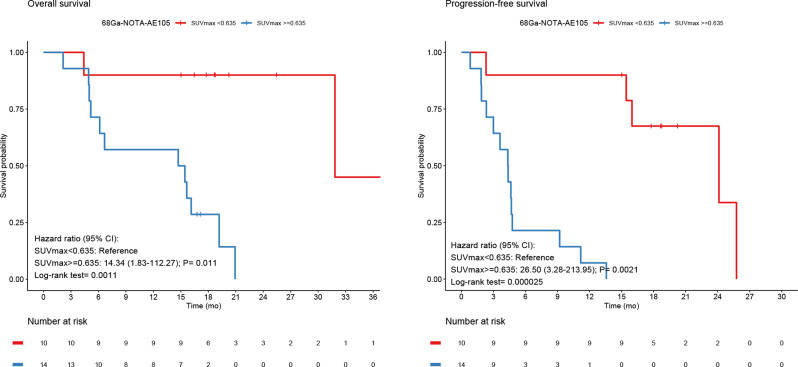
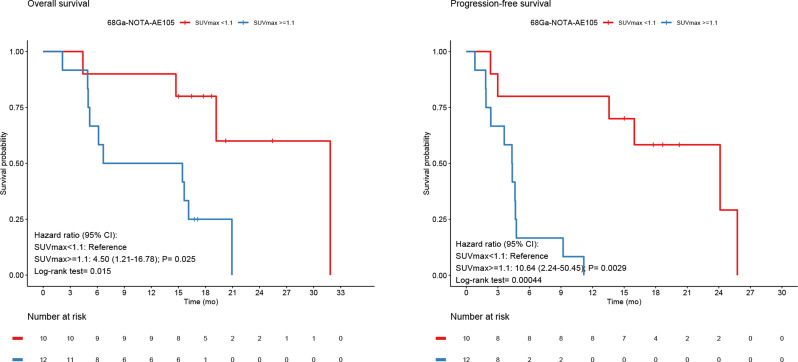
Methods: In a prospective phase II clinical trial, 24 patients suspected of primary glioma underwent a dynamic 60-min PET/MRI following the administration of approximately 200 MBq (range: 83-222 MBq) [68Ga]Ga-NOTA-AE105. Lesions were considered uPAR positive if the tumor-to-background ratio, calculated as the ratio of TumorSUVmax-to-Normal-BrainSUVmean tumor-SUVmax-to-background-SUVmean, was ≥ 2.0. The patients were followed over time to assess OS and PFS and stratified into high and low uPAR expression groups based on TumorSUVmax.
Results: Of the 24 patients, 16 (67%) were diagnosed with WHO grade 4 gliomas, 6 (25%) with grade 3, and 2 (8%) with grade 2. Two-thirds of all patients (67%) presented with uPAR positive lesions and 94% grade 4 gliomas. At median follow up of 18.8 (2.1-45.6) months, 19 patients had disease progression and 14 had died. uPAR expression dichotomized into high and low, revealed significant worse prognosis for the high uPAR group for OS and PFS with HR of 14.3 (95% CI, 1.8-112.3; P = 0.011), and HR of 26.5 (95% CI, 3.3-214.0; P = 0.0021), respectively. uPAR expression as a continuous variable was associated with worse prognosis for OS and PFS with HR of 2.7 (95% CI, 1.5-4.8; P = 0.0012), and HR of 2.5 (95% CI, 1.5-4.2; P = 0.00073), respectively.
Conclusions: The majority of glioma patients and almost all with grade 4 gliomas displayed uPAR positive lesions underlining the feasibility of 68Ga-NOTA-AE105 PET/MRI in gliomas. High uPAR expression is significantly correlated with worse survival outcomes for patients. Additionally, the high proportion of uPAR positive gliomas underscores the potential of uPAR-targeted radionuclide therapy in these patients.
Trail registration: EudraCT No: 2016-002417-21; the Scientific Ethics Committee: H-16,035,303; the Danish Data Protection Agency: 2012-58-0004; clinical trials registry: NCT02945826, 26Oct2016, URL: https://classic.
Clinicaltrials: gov/ct2/show/NCT02945826 .
Keywords: Glioma; Molecular imaging; PET/MRI; Prognosis; Targeted radionuclide therapy; Urokinase plasminogen activator receptor (uPAR).
© 2024. The Author(s).
Conflict of interest statement
AK is an inventor on a patent of the composition of matter used in the study and a co-founder of Curasight that seeks to commercialize uPAR-PET. The current study is an academic investigator-initiated trial. No other potential conflicts of interest relevant are to this article exist.
Figures
References
Associated data
Grants and funding
- Lundbeck Foundation/Lundbeck Foundation
- Novo Nordisk Fonden/Novo Nordisk Fonden
- Innovationsfonden/Innovationsfonden
- Neuroendocrine Tumor Research Foundation/Neuroendocrine Tumor Research Foundation
- Kræftens Bekæmpelse/Kræftens Bekæmpelse
- Arvid Nilssons Fond/Arvid Nilssons Fond
- The Neye Foundation/The Neye Foundation
- The Sygeforsikringen Danmark/The Sygeforsikringen Danmark
- The Research Foundation of Rigshospitalet/The Research Foundation of Rigshospitalet
- The Danish National Research Foundation - PERSEMONE/The Danish National Research Foundation - PERSEMONE
- The Research Council of the Capital Region of Denmark/The Research Council of the Capital Region of Denmark
- The Danish Health Authority/The Danish Health Authority
- The John and Birthe Meyer Foundation/The John and Birthe Meyer Foundation
- Danmarks Frie Forskningsfond/Danmarks Frie Forskningsfond
- 670261/H2020 European Institute of Innovation and Technology
- 668532/H2020 European Institute of Innovation and Technology
LinkOut - more resources
Full Text Sources
Medical
