

An anthropomorphic phantom for atrial transseptal puncture simulation training
- PMID: 39472399
- PMCID: PMC11523608
- DOI: 10.1186/s41205-024-00241-y
An anthropomorphic phantom for atrial transseptal puncture simulation training
Abstract
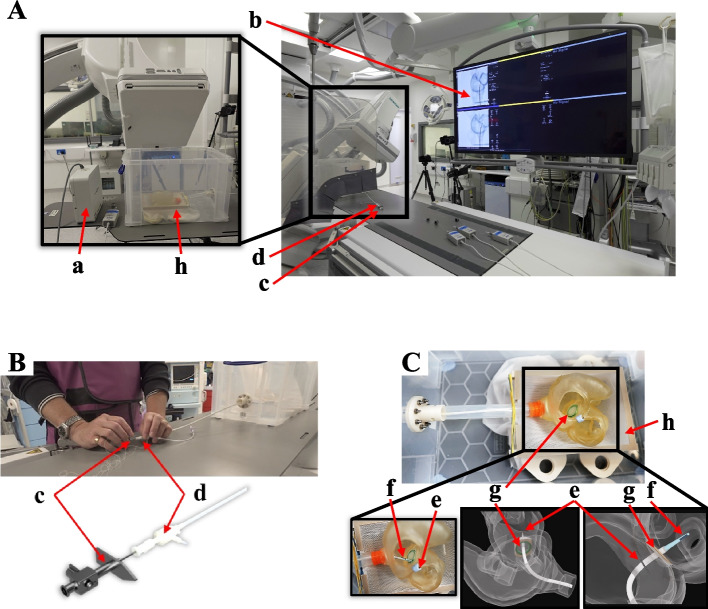
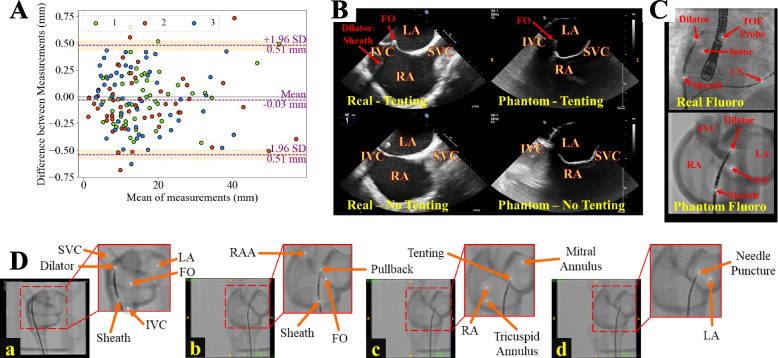
Background: Transseptal puncture (TSP) is a critical prerequisite for left-sided cardiac interventions, such as atrial fibrillation (AF) ablation and left atrial appendage closure. Despite its routine nature, TSP can be technically demanding and carries a risk of complications. This study presents a novel, patient-specific, anthropomorphic phantom for TSP simulation training that can be used with X-ray fluoroscopy and ultrasound imaging.
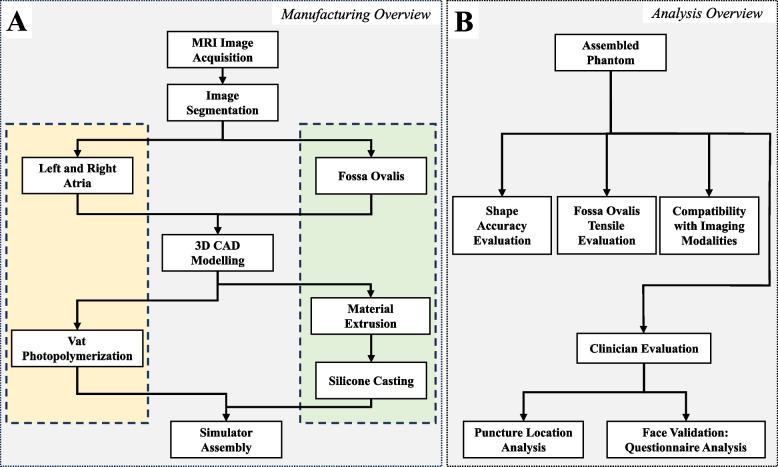
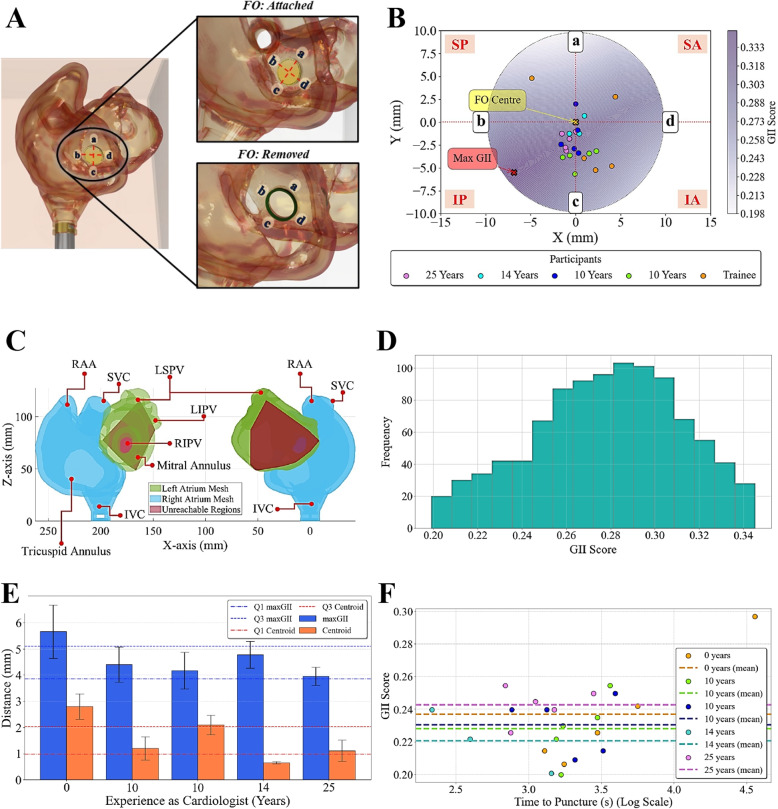
Methods: The TSP phantom was developed using additive manufacturing techniques and features a replaceable fossa ovalis (FO) component to allow for multiple punctures without replacing the entire model. Four cardiologists and one cardiology trainee performed TSP on the simulator, and their performance was assessed using four metrics: global isotropy index, distance from the centroid, time taken to perform TSP, and a set of 5-point Likert scale questions to evaluate the clinicians' perception of the phantom's realism and utility.
Results: The results demonstrate the simulator's potential as a training tool for interventional cardiology, providing a realistic and controllable environment for clinicians to refine their TSP skills. Experienced cardiologists tended to cluster their puncture points closer to regions of the FO associated with higher global isotropy index scores, indicating a relationship between experience and optimal puncture localization. The questionnaire analysis revealed that participants generally agreed on the phantom's realistic anatomical representation and ability to accurately visualize the TSP site under fluoroscopic guidance.
Conclusions: The TSP simulator can be incorporated into training programs, offering trainees the opportunity to improve tool handling, spatial coordination, and manual dexterity prior to performing the procedure on patients. Further studies with larger sample sizes and longitudinal assessments are needed to establish the simulator's impact on TSP performance and patient outcomes.
Keywords: 3D printing; Cardiology; Patient-specific; Simulation; Training; Transseptal puncture.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- De Ponti R, Marazzi R, Ghiringhelli S, Salerno-Uriarte JA, Calkins H, Cheng A. Superiority of simulator-based training compared with conventional training methodologies in the performance of transseptal catheterization. J Am Coll Cardiol. 2011;58(4):359–63. - PubMed
-
- Alkhouli M, Rihal CS, Holmes DR. Transseptal techniques for emerging structural heart interventions. JACC Cardiovasc Interv. 2016;9(24):2465–80. - PubMed
Grants and funding
- WT_/Wellcome Trust/United Kingdom
- WT203148/Z/16/Z/Wellcome Centre for Medical Engineering at King's College London
- MIC-2016-019/Department of Health and Social Care (DHSC) through the National Institute for Health and Care Research (NIHR) MedTech and Vitro Diagnostic Co-operative (MIC) award for Cardiovascular Diseases to Guy's & St Thomas' NHS Foundation Trust in partnership with King's College London
LinkOut - more resources
Full Text Sources
Miscellaneous