

Outcomes of Balloon-Expandable Transcatheter Aortic Valve Replacement in Younger Patients in the Low-Risk Era
- PMID: 39475333
- PMCID: PMC11525662
- DOI: 10.1001/jamacardio.2024.4237
Outcomes of Balloon-Expandable Transcatheter Aortic Valve Replacement in Younger Patients in the Low-Risk Era
Erratum in
-
Error in Figure.JAMA Cardiol. 2025 Feb 1;10(2):201. doi: 10.1001/jamacardio.2024.4925. JAMA Cardiol. 2025. PMID: 39630461 Free PMC article. No abstract available.
-
Error in Abstract and Results.JAMA Cardiol. 2025 Feb 1;10(2):202. doi: 10.1001/jamacardio.2025.0009. JAMA Cardiol. 2025. PMID: 39937198 Free PMC article. No abstract available.
Abstract
Importance: Guidelines advise heart team assessment for all patients with aortic stenosis, with surgical aortic valve replacement recommended for patients younger than 65 years or with a life expectancy greater than 20 years. If bioprosthetic valves are selected, repeat procedures may be needed given limited durability of tissue valves; however, younger patients with aortic stenosis may have major comorbidities that can limit life expectancy, impacting decision-making.
Objective: To characterize patients younger than 65 years who received transcatheter aortic valve replacement (TAVR) and compare their outcomes with patients aged 65 to 80 years.
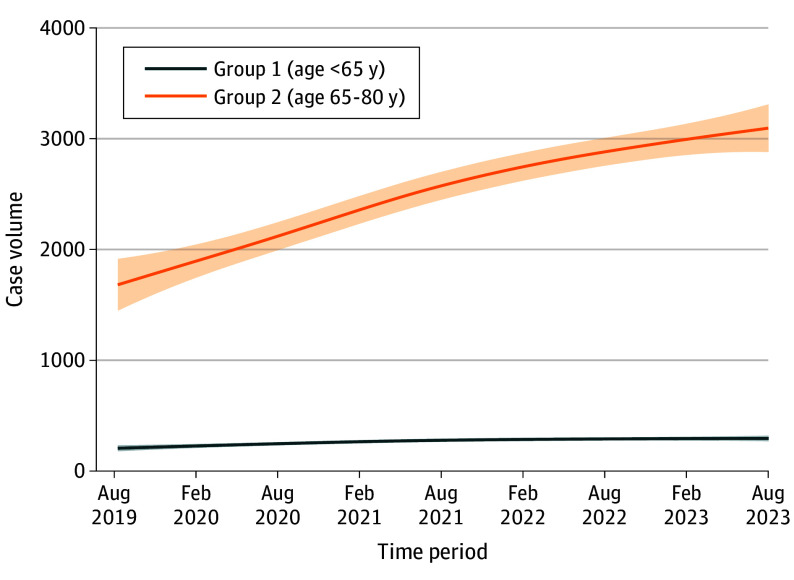
Design, setting, and participants: This retrospective registry-based analysis used data on 139 695 patients from the Society for Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy (TVT) Registry, inclusive of patients 80 years and younger undergoing TAVR from August 2019 to September 2023.
Intervention: Balloon-expandable valve (BEV) TAVR with the SAPIEN family of devices.
Main outcomes and measures: Comorbidities (heart failure, coronary artery disease, dialysis, and others) and outcomes (death, stroke, and hospital readmission) of patients younger than 65 years compared to patients aged 65 to 80 years.
Results: In the years surveyed, 13 849 registry patients (5.7%) were younger than 65 years, 125 846 (52.1%) were aged 65 to 80 years, and 101 725 (42.1%) were 80 years and older. Among those younger than 65, the mean (SD) age was 59.7 (4.8) years, and 9068 of 13 849 patients (65.5%) were male. Among those aged 65 to 80 years, the mean (SD) age was 74.1 (4.2) years, and 77 817 of 125 843 patients (61.8%) were male. Those younger than 65 years were more likely to have a bicuspid aortic valve than those aged 65 to 80 years (3472/13 755 [25.2%] vs 9552/125 001 [7.6%], respectively; P < .001). They were more likely to have congestive heart failure, chronic lung disease, diabetes, immunocompromise, and end stage kidney disease receiving dialysis. Patients younger than 65 years had worse baseline quality of life (mean [SD] Kansas City Cardiomyopathy Questionnaire score, 47.7 [26.3] vs 52.9 [25.8], respectively; P < .001) and mean (SD) gait speed (5-meter walk test, 6.6 [5.8] seconds vs 7.0 [4.9] seconds, respectively; P < .001) than those aged 65 to 80 years. At 1 year, patients younger than 65 years had significantly higher readmission rates (2740 [28.2%] vs 23 178 [26.1%]; P < .001) and all-cause mortality (908 [9.9%] vs 6877 [8.2%]; P < .001) than older patients. When propensity matched, younger patients still had higher 1-year readmission rates (2732 [28.2%] vs 2589 [26.8%]; P < .03) with similar mortality to their older counterparts (905 [9.9%] vs 827 [10.1%]; P = .55).
Conclusions and relevance: Among US patients receiving BEV TAVR for severe aortic stenosis in the low-surgical risk era, those younger than 65 years represent a small subset. Patients younger than 65 years had a high burden of comorbidities and incurred higher rates of death and readmission at 1 year compared to their older counterparts. These observations suggest that heart team decision-making regarding TAVR for most patients in this age group is clinically valid.
Conflict of interest statement
Figures

Comment on
-
TAVR in Young Patients With Aortic Stenosis: Appropriate Use or Indication Creep?JAMA Cardiol. 2025 Feb 1;10(2):136. doi: 10.1001/jamacardio.2024.4300. JAMA Cardiol. 2025. PMID: 39475343 No abstract available.
References
-
- Otto CM, Nishimura RA, Bonow RO, et al. ; Writing Committee Members . 2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021;77(4):450-500. doi: 10.1016/j.jacc.2020.11.035 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
