

Initial blood pressure and adverse cardiac events following acute ischaemic stroke: An individual patient data pooled analysis from the VISTA database
- PMID: 39475369
- PMCID: PMC11556537
- DOI: 10.1177/23969873241296391
Initial blood pressure and adverse cardiac events following acute ischaemic stroke: An individual patient data pooled analysis from the VISTA database
Abstract
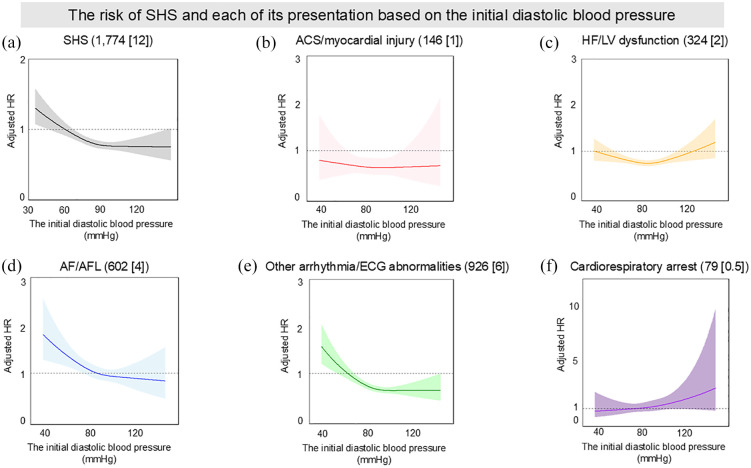
Background: Adverse cardiac events following ischaemic stroke (stroke-heart syndrome, SHS) pose a clinical challenge. We investigated the association between initial blood pressure at stroke presentation and the risk of SHS.
Methods: We utilised data from the Virtual International Stroke Trials Archive (VISTA). We defined SHS as the incidence of cardiac complications within 30 days post-ischaemic stroke. These presentations included acute coronary syndrome encompassing myocardial injury, heart failure/left ventricular dysfunction, atrial fibrillation/flutter, other arrhythmia/electrocardiogram abnormalities, and cardiorespiratory arrest. Using Cox proportional hazards models, we assessed the risk trajectories for developing SHS and its presentations associated with initial blood pressure. We also explored the risk trajectories for 90-day mortality related to initial blood pressure.
Results: From 16,095 patients with acute ischaemic stroke, 14,965 (mean age 69 ± 12 years; 55% male) were analysed. Of these, 1774 (11.8%) developed SHS. The risk of SHS and initial blood pressure showed a U-shaped relationship. The lowest blood pressures (⩽130 mmHg systolic and ⩽55 mmHg diastolic) were associated with the highest risks (adjusted hazard ratio [95%confidence interval]: 1.40 [1.21-1.63]; p < 0.001, 1.71 [1.39-2.10]; p < 0.001, respectively, compared to referential blood pressure range).Cardiorespiratory arrest posed the greatest risk at higher blood pressure levels (2.34 [1.16-4.73]; p = 0.017 for systolic blood pressure >190 mmHg), whereas other presentations exhibited the highest risk at lower pressures. The 90-day mortality risk also followed a U-shaped distribution, with greater risks observed at high blood pressure thresholds.
Conclusions: There is a U-shaped relationship between initial blood pressure at ischaemic stroke presentation and the risk of subsequent SHS.
Keywords: Ischaemic stroke; blood pressure; stroke-heart syndrome.
Conflict of interest statement
Declaration of conflicting interestThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HI, BH, WKE, JD and AHAR report no conflicts of interest.GYHL reports Consultant and speaker for BMS/Pfizer, Boehringer Ingelheim, Daiichi-Sankyo, Anthos. No fees are received personally. He is a National Institute for Health and Care Research (NIHR) Senior Investigator and co-PI of the AFFIRMO project on multimorbidity in AF (grant agreement No 899871), TARGET project on digital twins for personalised management of atrial fibrillation and stroke (grant agreement No 101136244) and ARISTOTELES project on artificial intelligence for management of chronic long term conditions (grant agreement No 101080189), which are all funded by the EU’s Horizon Europe Research & Innovation programme.
Figures




References
-
- Prosser J, MacGregor L, Lees KR, et al.; VISTA Investigators. Predictors of early cardiac morbidity and mortality after ischemic stroke. Stroke 2007; 38: 2295–2302. - PubMed
-
- Sposato LA, Hilz MJ, Aspberg S, et al.; World Stroke Organisation Brain & Heart Task Force. Post-stroke cardiovascular complications and neurogenic cardiac injury: JACC state-of-the-art review. J Am Coll Cardiol 2020; 76: 2768–2785. - PubMed
-
- Buckley BJR, Harrison SL, Lane DA, et al. Stroke-heart syndrome: mechanisms, risk factors, and adverse cardiovascular events. Eur J Prev Cardiol 2024; 31: e23–e26. - PubMed
-
- Scheitz JF, Nolte CH, Doehner W, et al. Stroke-heart syndrome: clinical presentation and underlying mechanisms. Lancet Neurol 2018; 17: 1109–1120. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
