

Pretreatment With Unfractionated Heparin in ST-Elevation Myocardial Infarction—A Propensity Score Matching Analysis
- PMID: 39475751
- PMCID: PMC12094712
- DOI: 10.3238/arztebl.m2024.0212
Pretreatment With Unfractionated Heparin in ST-Elevation Myocardial Infarction—A Propensity Score Matching Analysis
Abstract
Background: Patients with ST-segment elevation myocardial infarction (STEMI) are often pretreated with unfractionated heparin (UFH) before a primary percutaneous coronary intervention (PPCI). UFH pretreatment is intended to lessen the thrombotic burden, but there have been conflicting study findings on its safety and efficacy. We assessed the risks and benefits of UFH pretreatment with a retrospective analysis of registry data from the STEMI network of a German metropolitan region.
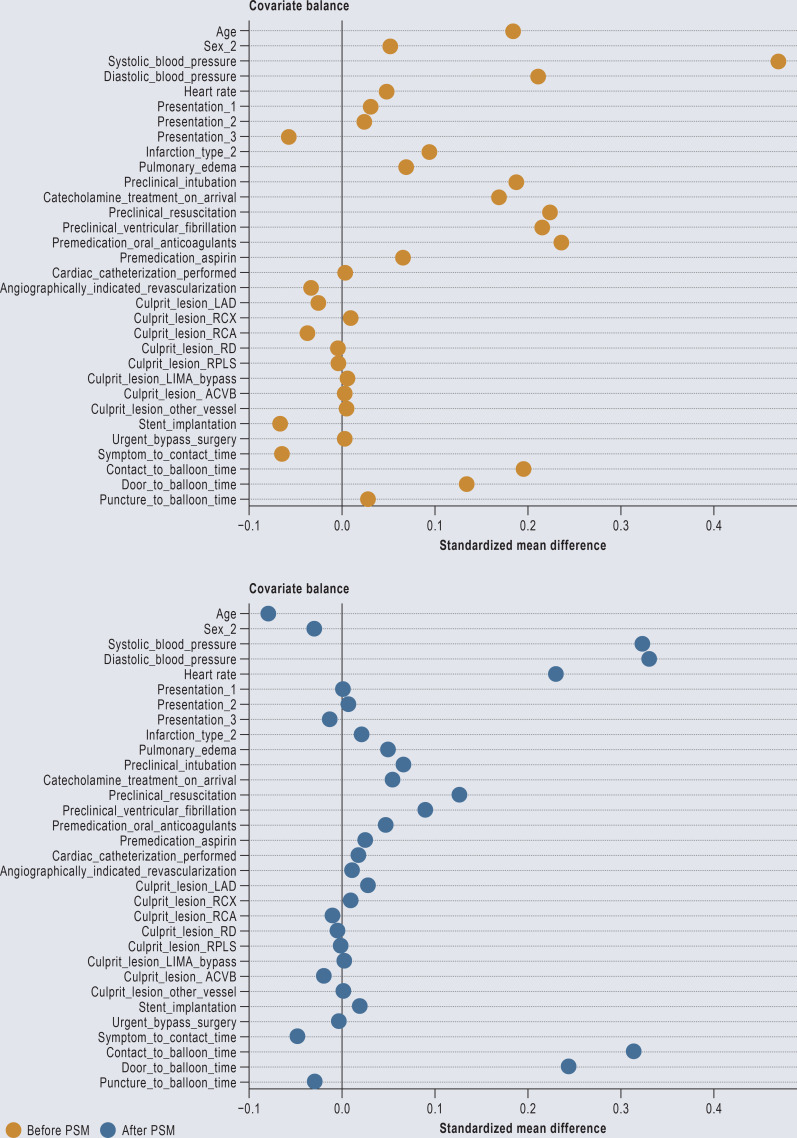
Methods: Data from patients with STEMI referred for PPCI from 2005 to 2020 were evaluated with an adjusted outcome analysis, including propensity score matching (PSM). The endpoints included the patency of the infarct-related artery (IRA) after PPCI, in-hospital mortality, access-site bleeding, and the peak creatine kinase (CK) level.
Results: We assessed data from 4632 patients with STEMI: 4420 (95.4%) were pretreated with UFH, and 212 (4.6%) were not. After PSM of 511 vs. 187 patients, the adjusted odds ratios for the various endpoints were (pretreatment vs. no pretreatment, with 95% confidence intervals): for impaired flow of the IRA, 1.01 [0.59; 1.74]; for in-hospital mortality, 1.46 [0.88; 2.42]; and for access-site bleeding, 0.59 [0.14; 2.46]. The peak creatine kinase levels were similar in the two groups (median, 1248.0 vs. 1376.5 U/L, estimated difference -134 [-611; 341]).
Conclusion: UFH pretreatment was less frequently performed in STEMI patients who had undergone cardiopulmonary resuscitation. UFH pretreatment was not associated with increased access-site bleeding, nor was it found to have significantly higher efficacy with respect to the relevant endpoints. The risks and benefits of UFH pretreatment should be weighed individually in each case, as evidence from high-quality clinical trials is lacking. Data from the existing literature suggest that no pretreatment is an option to be considered, as are certain alternative antithrombotic strategies.
Figures


References
-
- Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44:3720–3826. - PubMed
-
- Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2018;39:119–177. - PubMed
-
- O‘Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127 e362-425. - PubMed
-
- Karlsson S, Andell P, Mohammad MA, et al. Editor‘s Choice- Heparin pre-treatment in patients with ST-segment elevation myocardial infarction and the risk of intracoronary thrombus and total vessel occlusion. Insights from the TASTE trial. Eur Heart J Acute Cardiovasc Care. 2019;8:15–23. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous