

Combined analysis of the MF18-02/MF18-03 NEOSENTITURK studies: ypN-positive disease does not necessitate axillary lymph node dissection in patients with breast cancer with a good response to neoadjuvant chemotherapy as long as radiotherapy is provided
- PMID: 39476303
- PMCID: PMC11694236
- DOI: 10.1002/cncr.35610
Combined analysis of the MF18-02/MF18-03 NEOSENTITURK studies: ypN-positive disease does not necessitate axillary lymph node dissection in patients with breast cancer with a good response to neoadjuvant chemotherapy as long as radiotherapy is provided
Abstract
Background: The omission of axillary lymph node dissection (ALND) remains controversial for patients with residual axillary disease after neoadjuvant chemotherapy (NAC), regardless of the residual burden. This study evaluated the oncologic safety and factors associated with outcomes in patients with residual axillary disease. These patients were treated solely with sentinel lymph node biopsy (SLNB) or targeted axillary dissection (TAD), without ALND, after NAC.
Methods: A joint analysis of two different multicenter cohorts-the retrospective cohort registry MF18-02 and the prospective observational cohort registry MF18-03 (NCT04250129)-was conducted between January 2004 and August 2022. All patients received regional nodal irradiation.
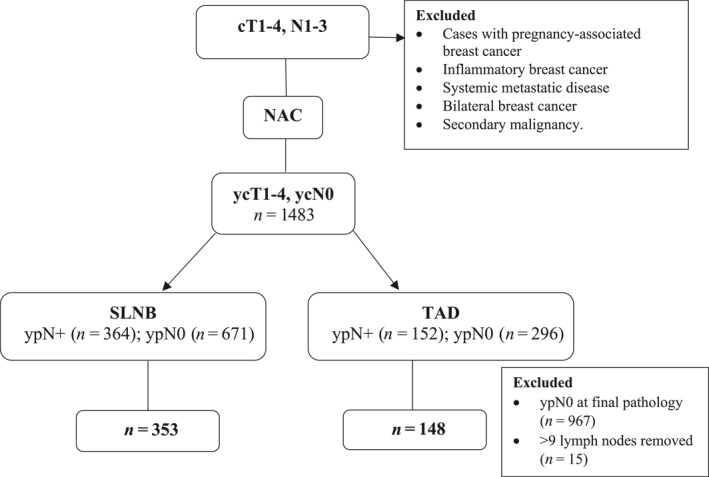
Results: Five hundred and one patients with cT1-4, N1-3M0 disease who achieved a complete clinical response to NAC underwent either SLNB alone (n = 353) or TAD alone (n = 148). At a median follow-up of 42 months, axillary and locoregional recurrence rates were 0.4% (n = 2) and 0.8% (n = 4). No significant difference was found in disease-free survival (DFS) and disease-specific survival (DSS) rates between patients undergoing TAD alone versus SLNB alone, those with breast positive versus negative pathologic complete response, SLN methodology, total metastatic LN of one versus ≥2, or metastasis types as isolated tumor cells with micrometastases versus macrometastases. In the multivariate analysis, patients with nonluminal pathology were more likely to have a worse DFS and DSS, respectively, without an increased axillary recurrence.
Conclusions: The omission of ALND can be safely considered for patients who achieve a complete clinical response after NAC, even if residual disease is detected by pathologic examination. Provided that adjuvant radiotherapy is administered, neither the SLNB method nor the number of excised LNs significantly affects oncologic outcomes.
Keywords: axillary lymph node dissection; breast cancer; neoadjuvant chemotherapy; sentinel lymph node biopsy; targeted axillary dissection.
© 2024 The Author(s). Cancer published by Wiley Periodicals LLC on behalf of American Cancer Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Giuliano AE, Ballman K, McCall L, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: long‐term follow‐up from the American College of Surgeons Oncology Group (Alliance) ACOSOG Z0011 randomized trial. Ann Surg. 2016;264(3):413‐420. doi: 10.1097/SLA.0000000000001863 - DOI - PMC - PubMed
-
- Giuliano AE, Ballman KV, McCall L, et al. Effect of axillary dissection vs no axillary dissection on 10‐year overall survival among women with invasive breast cancer and sentinel node metastasis: the ACOSOG Z0011 (Alliance) randomized clinical trial. JAMA. 2017;318(10):918‐926. doi: 10.1001/jama.2017.11470 - DOI - PMC - PubMed
-
- Donker M, van Tienhoven G, Straver ME, et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981‐22023 AMAROS): a randomized, multicentre, open‐label, phase 3 non‐inferiority trial. Lancet Oncol. 2014;15(12):1303‐1310. doi: 10.1016/S1470-2045(14)70460-7 - DOI - PMC - PubMed
-
- Bartels SAL, Donker M, Poncet C, et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer: 10‐year results of the randomized controlled EORTC 10981‐22023 AMAROS trial. J Clin Oncol. 2023;41(12):2159‐2165. - PubMed
-
- Galimberti V, Cole BF, Viale G, et al. Axillary dissection versus no axillary dissection in patients with breast cancer and sentinel‐node micrometastases (IBCSG 23‐01): 10‐year follow‐up of a randomised, controlled phase 3 trial. Lancet Oncol. 2018;19(10):1385‐1393. doi: 10.1016/S1470-2045(18)30380-2 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
