

Variation in the detection of lymphovascular invasion in T1 colorectal cancer and its impact on treatment: A nationwide Dutch study
- PMID: 39476327
- PMCID: PMC11652325
- DOI: 10.1002/ueg2.12670
Variation in the detection of lymphovascular invasion in T1 colorectal cancer and its impact on treatment: A nationwide Dutch study
Abstract
Background: Lymphovascular invasion (LVI) plays an important role in determining the risk of lymph node metastasis (LNM) in T1 colorectal cancer (CRC) patients and influencing treatment decisions and patient outcomes.
Objective: This study evaluated how the detection of LVI varies between Dutch laboratories and investigated its impact on the treatment and oncological outcomes of T1 CRC patients.
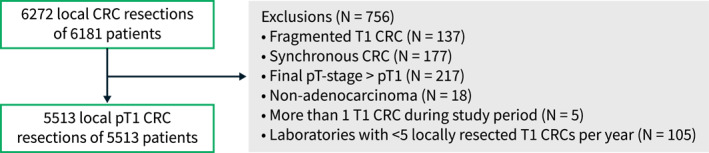
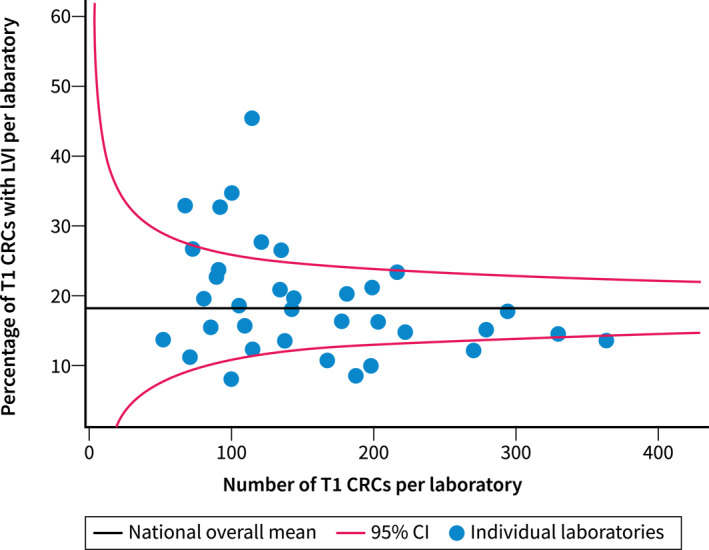
Methods: Pathology reports and clinical data of T1 CRC patients who underwent local resection between 2015 and 2019 were obtained from the Dutch nationwide pathology databank (Palga cohort, n = 5513). Data on the standard of LVI diagnosis (H&E/Immunohistochemistry) were not available. We categorized laboratories as low, average, or high detectors and evaluated the impact of LVI detection practice on the surgical resection rate and the proportion of LNM-negative (LNM-) surgeries. In the second part of the study, we used the Dutch T1 CRC Working Group cohort (n = 1268) to evaluate the impact of LVI detection practice on cancer recurrences during follow-up. Multivariable logistic regression analyses and Cox proportional hazard regression were used to study the association between LVI detection practice and the outcomes.
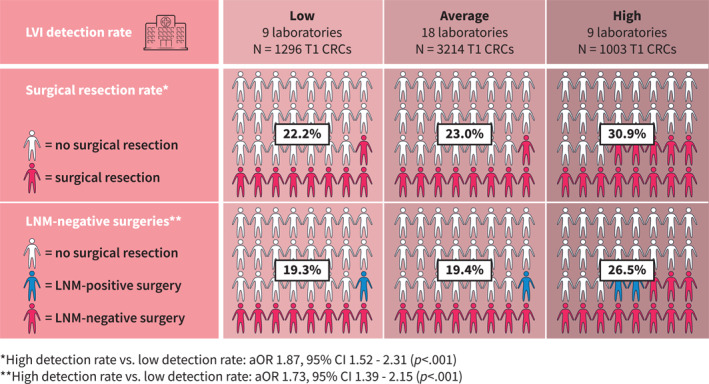
Results: In the PALGA cohort, the proportion of surgical resections after local resection of a T1 CRC was significantly higher among patients diagnosed by laboratories with a high LVI detection rate (high vs. low: adjusted OR [aOR] 1.87; 95% confidence interval [CI] 1.52-2.31) as was the proportion of LNM-surgeries (aOR 1.73; 95% CI 1.39-2.15). In the second cohort, no significant difference was observed in cancer recurrences among patients diagnosed in laboratories with high detection rates compared with low detection rates (aHR 2.23; 95% CI 0.94-5.23).
Conclusion: These findings suggest that a high detection rate of LVI does not improve oncological outcomes and may expose more patients to unnecessary oncological surgery, emphasizing the need for standardization of LVI diagnosis.
Keywords: CRC; bowel; histology; intestine; lymph node; metastasis; neoplasia; outcomes; stadiation; therapy.
© 2024 The Author(s). United European Gastroenterology Journal published by Wiley Periodicals LLC on behalf of United European Gastroenterology.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Bosch S, Teerenstra S, De Wilt JW, Cunningham C, Nagtegaal I. Predicting lymph node metastasis in pT1 colorectal cancer: a systematic review of risk factors providing rationale for therapy decisions. Endoscopy. 2013;45(10):827–834. [Internet]. [Cited 2020 Jul 27]. 10.1055/s-0033-1344238 - DOI - PubMed
-
- Kajiwara Y, Oka S, Tanaka S, Nakamura T, Saito S, Fukunaga Y, et al. Nomogram as a novel predictive tool for lymph node metastasis in T1 colorectal cancer treated with endoscopic resection: a nationwide, multicenter study. Gastrointest Endosc. 2023;97(6):1119–1128.e5. [Internet]. 10.1016/j.gie.2023.01.022 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
