

The impact of short-course total neoadjuvant therapy, long-course chemoradiotherapy, and upfront surgery on the technical difficulty of total mesorectal excision: an observational study with an intraoperative perspective
- PMID: 39477330
- PMCID: PMC11532385
- DOI: 10.3393/ac.2023.00899.0128
The impact of short-course total neoadjuvant therapy, long-course chemoradiotherapy, and upfront surgery on the technical difficulty of total mesorectal excision: an observational study with an intraoperative perspective
Abstract
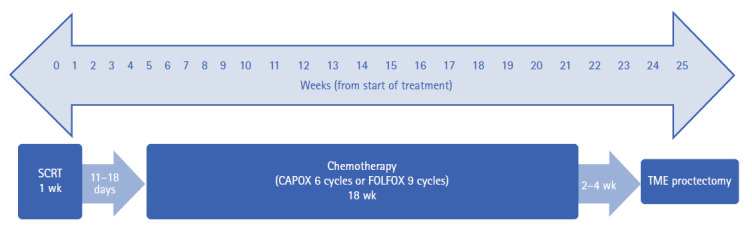
Purpose: Total neoadjuvant therapy (TNT) is becoming the standard of care for locally advanced rectal cancer. However, surgery is deferred for months after completion, which may lead to fibrosis and increased surgical difficulty. The aim of this study was to assess whether TNT (TNT-RAPIDO) is associated with increased difficulty of total mesorectal excision (TME) compared with long-course chemoradiotherapy (LCRT) and upfront surgery.
Methods: Twelve laparoscopic videos of low anterior resection with TME for rectal cancer were prospectively collected from January 2020 to October 2021, with 4 videos in each arm. Seven colorectal surgeons assessed the videos independently, graded the difficulty of TME using a visual analog scale and attempted to identify which category the videos belonged to.
Results: The median age was 67 years, and 10 patients were male. The median interval to surgery from radiotherapy was 13 weeks in the LCRT group and 24 weeks in the TNT-RAPIDO group. There was no significant difference in the visual analog scale for difficulty in TME between the 3 groups (LCRT, 3.2; TNT-RAPIDO, 4.6; upfront, 4.1; P=0.12). A subgroup analysis showed similar difficulty between groups (LCRT 3.2 vs. TNT-RAPIDO 4.6, P=0.05; TNT-RAPIDO 4.6 vs. upfront 4.1, P=0.54). During video assessments, surgeons correctly identified the prior treatment modality in 42% of the cases. TNT-RAPIDO videos had the highest recognition rate (71%), significantly outperforming both LCRT (29%) and upfront surgery (25%, P=0.01).
Conclusion: TNT does not appear to increase the surgical difficulty of TME.
Keywords: Minimally invasive surgical procedures; Neoadjuvant therapy; Radiotherapy; Rectal neoplasms; Surgical difficulty.
Conflict of interest statement
Frederick H. Koh is an Editorial Board member of
Figures
References
-
- Komen N, Dewint P, Van den Broeck S, Pauli S, de Schepper H. Rectal cancer surgery: what’s in a name? Acta Gastroenterol Belg. 2019;82:67–74. - PubMed
-
- van Gijn W, Marijnen CA, Nagtegaal ID, Kranenbarg EM, Putter H, Wiggers T, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomized controlled TME trial. Lancet Oncol. 2011;12:575–82. - PubMed
-
- Sauer R, Liersch T, Merkel S, Fietkau R, Hohenberger W, Hess C, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol. 2012;30:1926–33. - PubMed
-
- Ma B, Gao P, Wang H, Xu Q, Song Y, Huang X, et al. What has preoperative radio(chemo)therapy brought to localized rectal cancer patients in terms of perioperative and long-term outcomes over the past decades? A systematic review and meta-analysis based on 41,121 patients. Int J Cancer. 2017;141:1052–65. - PubMed
LinkOut - more resources
Full Text Sources
