

Inflammasome-targeted therapy might prevent adverse perinatal outcomes of recurrent chronic intervillositis of unknown etiology
- PMID: 39477918
- PMCID: PMC11525837
- DOI: 10.1038/s41467-024-53591-w
Inflammasome-targeted therapy might prevent adverse perinatal outcomes of recurrent chronic intervillositis of unknown etiology
Abstract
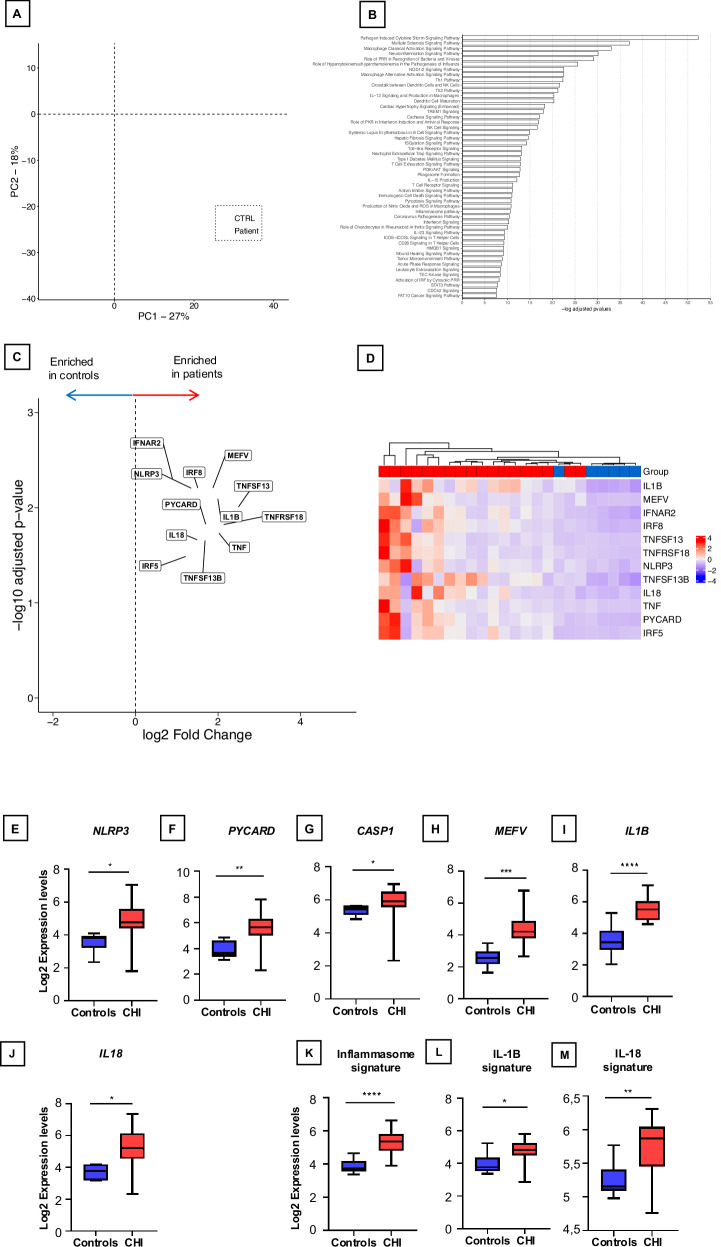
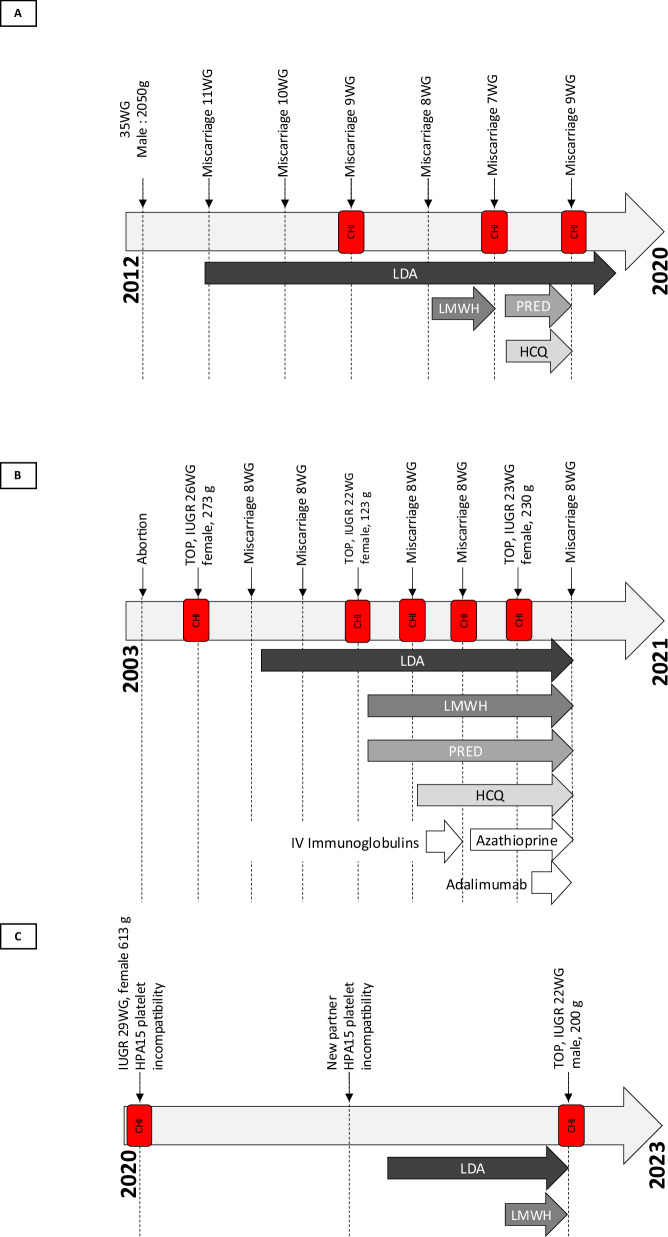
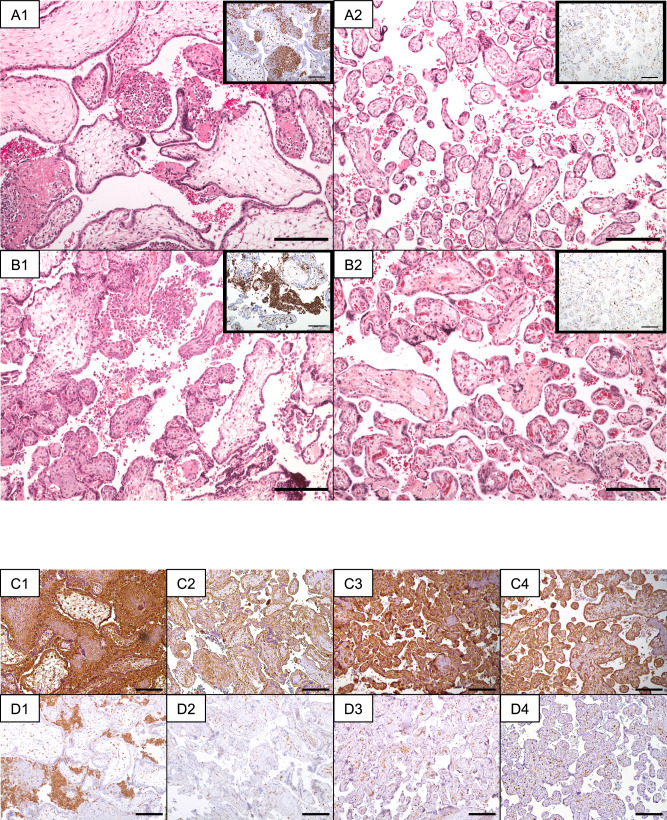
Chronic histiocytic intervillositis of unknown origin (CHI) is a rare placental disorder associated with adverse pregnancy outcomes, frequent recurrence, and a lack of effective preventive strategies. Recent insights indicate a potential link between CHI-associated inflammatory lesions and the inflammasome pathway, suggesting innovative therapeutic avenues. Here we show a potential role of the inflammasome pathway in CHI through comprehensive transcriptomic analysis of grade 2 or 3 histopathologic CHI samples, paired with placental controls. Additionally, we present case studies of three individuals with recurrent CHI, who have undergone treatment with anakinra and colchicine throughout pregnancy, resulting in improved perinatal outcomes. Notably, all cases are characterized by the birth of healthy, full-term infants, with reduced or absent intervillositis recurrence. Placental assessment unveils heightened activation of the NLRP3-PYCARD inflammasome pathway and IL-1β processing in CHI samples, with downregulation observed in treated pregnancy samples, devoid of intervillositis. Collectively, these findings suggest a potential therapeutic role for targeting the inflammasome pathway in preventing recurrent CHI in pregnant individuals.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Understanding a Potential Role for the NLRP3 Inflammasome in Placenta-Mediated Pregnancy Complications.Am J Reprod Immunol. 2025 Apr;93(4):e70077. doi: 10.1111/aji.70077. Am J Reprod Immunol. 2025. PMID: 40260875 Free PMC article. Review.
-
Intravenous Immunoglobulins for Recurrent Chronic Histiocytic Intervillositis: A Series of Case Studies.Am J Reprod Immunol. 2024 Jul;92(1):e13898. doi: 10.1111/aji.13898. Am J Reprod Immunol. 2024. PMID: 38973779
-
Perinatal prognosis of pregnancies complicated by placental chronic villitis or intervillositis of unknown etiology and combined lesions: About a series of 178 cases.Placenta. 2016 Aug;44:104-8. doi: 10.1016/j.placenta.2016.04.017. Epub 2016 May 15. Placenta. 2016. PMID: 27452445
-
NLRP3 inflammasome function and pyroptotic cell death in human placental Hofbauer cells.J Reprod Immunol. 2020 Nov;142:103214. doi: 10.1016/j.jri.2020.103214. Epub 2020 Oct 3. J Reprod Immunol. 2020. PMID: 33152658 Free PMC article.
-
Recurrent Chronic Intervillositis: The Diagnostic Challenge - A Case Report and Review of the Literature.J Obstet Gynaecol Can. 2019 Mar;41(3):344-347. doi: 10.1016/j.jogc.2018.05.007. Epub 2018 Nov 7. J Obstet Gynaecol Can. 2019. PMID: 30414807 Review.
Cited by
-
Understanding a Potential Role for the NLRP3 Inflammasome in Placenta-Mediated Pregnancy Complications.Am J Reprod Immunol. 2025 Apr;93(4):e70077. doi: 10.1111/aji.70077. Am J Reprod Immunol. 2025. PMID: 40260875 Free PMC article. Review.
References
-
- Labarrere, C. & Mullen, E. Fibrinoid and trophoblastic necrosis with massive chronic intervillositis: an extreme variant of villitis of unknown etiology. Am. J. Reprod. Immunol. Microbiol15, 85–91 (1987). - PubMed
-
- Jacques, S. M. & Qureshi, F. Chronic intervillositis of the placenta. Arch. Pathol. Lab Med117, 1032–1035 (1993). - PubMed
-
- Parant, O., Capdet, J., Kessler, S., Aziza, J. & Berrebi, A. Chronic intervillositis of unknown etiology (CIUE): Relation between placental lesions and perinatal outcome. Eur. J. Obstet. Gynecol. Reprod. Biol.143, 9–13 (2009). - PubMed
-
- Marchaudon, V. et al. Chronic histiocytic intervillositis of unknown etiology: Clinical features in a consecutive series of 69 cases. Placenta32, 140–145 (2011). - PubMed
-
- Mekinian, A. et al. Chronic histiocytic intervillositis: Outcome, associated diseases and treatment in a multicenter prospective study. Autoimmunity48, 40–45 (2015). - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
