

Effect of therapeutic plasma exchange on tissue factor and tissue factor pathway inhibitor in septic shock
- PMID: 39478586
- PMCID: PMC11526504
- DOI: 10.1186/s13054-024-05142-4
Effect of therapeutic plasma exchange on tissue factor and tissue factor pathway inhibitor in septic shock
Abstract
Background: Coagulopathy is part of the pathological host response to infection in sepsis. Higher plasma concentrations of both tissue factor (TF) and tissue factor pathway inhibitor (TFPI) are associated with occurrence of disseminated intravascular coagulation (DIC), multi-organ dysfunction and increased mortality in patients with sepsis. Currently no treatment approaches specifically targeting this axis are available. We hypothesize that therapeutic plasma exchange (TPE) might limit this coagulopathy by restoring the balance of plasma proteins.
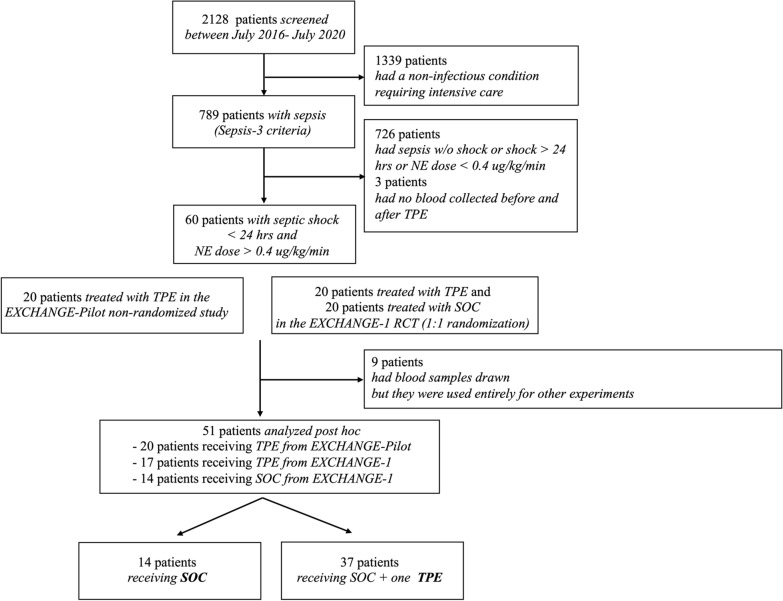
Methods: This was a pooled post-hoc biobank analysis including 51 patients with early (shock onset < 24 h) and severe (norepinephrine dose > 0.4 μg/kg/min) septic shock, who were either receiving standard of care treatment (SOC, n = 14) or SOC + one single TPE (n = 37). Plasma concentrations of TF and TFPI were measured both at- and 6 h after study inclusion. The effect of TPE on concentrations of TF and TFPI was investigated and compared to SOC patients. Further, baseline TF and TFPI concentrations were used to modulate and predict clinical response to adjunctive TPE, indicated by longitudinal reduction of lactate concentrations over the first 24 h following study inclusion.
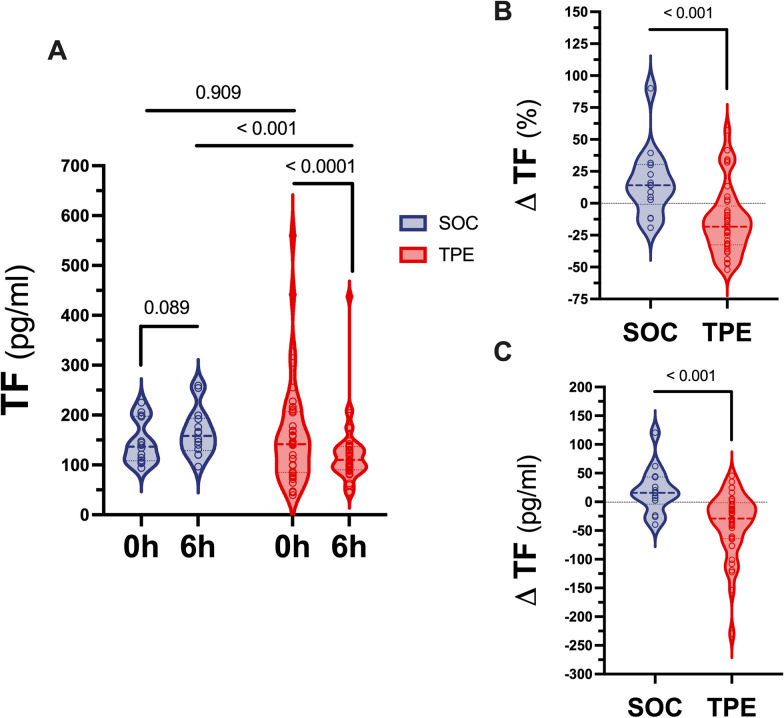
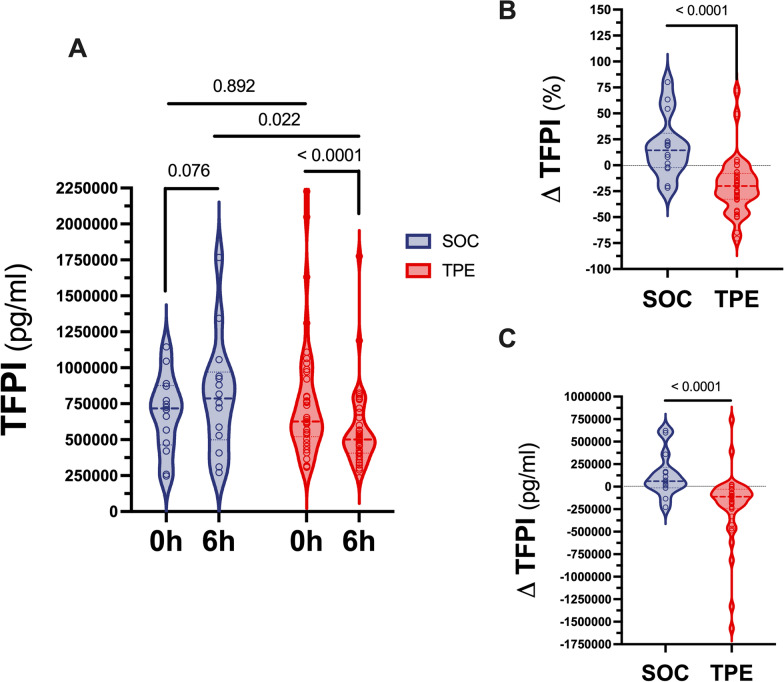
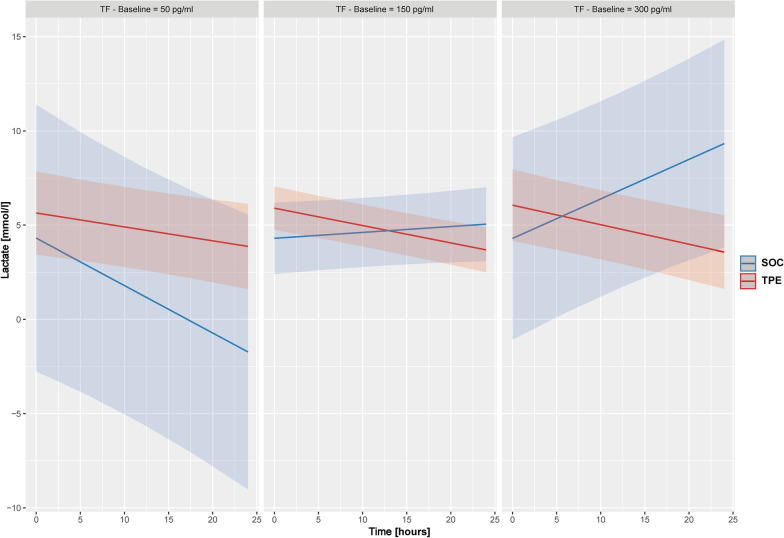
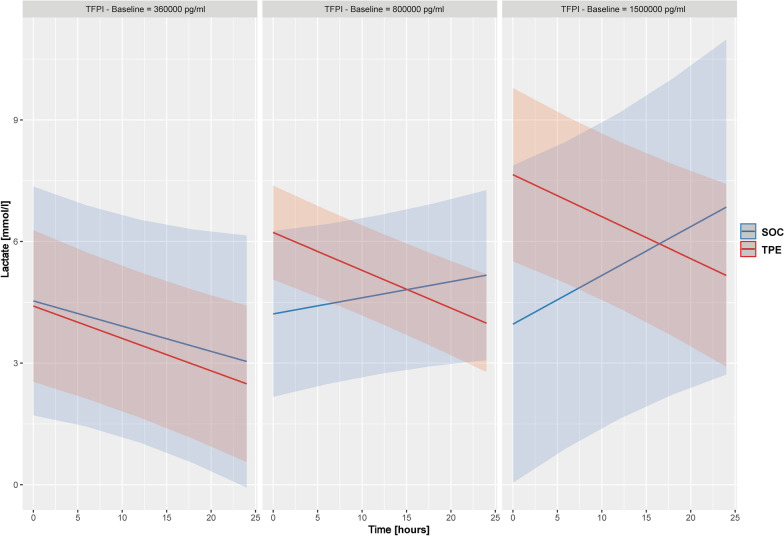
Results: TPE led to a significant reduction in circulating concentrations of both TF and TFPI while no difference was observed in the SOC group. Relative change of TF within 6 h was + 14 (-0.8 to + 30.4) % (p = 0.089) in the SOC and -18.3 (-32.6 to -2.2) % (p < 0.001) in the TPE group (between group p < 0.001). Similarly, relative change of TFPI was + 14.4 (-2.3 to + 30.9) % (p = 0.076) in the SOC and -20 (-32.8 to -7.9) % (p < 0.001) in the TPE group (between group p = 0.022). The ratio of TF to TFPI remained unchanged in both SOC and TPE groups. SOC patients exhibited an increase in lactate over the initial 24 h when TF and TFPI concentrations were higher at baseline. In contrast, patients undergoing TPE experienced a sustained longitudinal reduction of lactate concentrations across all levels of baseline TF and TFPI elevations. In a multivariate mixed-effects model, higher baseline TF (p = 0.003) and TFPI (p = 0.053) levels led to greater longitudinal lactate concentration reduction effects in the TPE group.
Conclusions: Adjunctive TPE in septic shock is associated with a significant removal of both TF and TFPI, which may contribute to the early hemodynamic improvement observed in septic shock patients receiving TPE. Higher baseline TF (and TFPI) plasma concentrations were identified as a putative predictor of treatment response that could be useful for predictive enrichment strategies in future clinical trials.
Keywords: Apheresis; Coagulation; Extracorporeal treatment; Plasmapheresis; Precision medicine; Sepsis; Tissue factor; Tissue factor pathway inhibitor.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Steinhagen F, Schmidt SV, Schewe JC, Peukert K, Klinman DM, Bode C. Immunotherapy in sepsis - brake or accelerate? Pharmacol Ther. 2020;208: 107476. - PubMed
-
- Engel C, Brunkhorst FM, Bone HG, Brunkhorst R, Gerlach H, Grond S, et al. Epidemiology of sepsis in Germany: results from a national prospective multicenter study. Intensive Care Med. 2007;33(4):606–18. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
