

Mapping and ablation of ventricular tachycardia using dual-energy lattice-tip focal catheter: early feasibility and safety study
- PMID: 39478679
- PMCID: PMC11577951
- DOI: 10.1093/europace/euae275
Mapping and ablation of ventricular tachycardia using dual-energy lattice-tip focal catheter: early feasibility and safety study
Abstract
Aims: Catheter ablation is an effective treatment method for recurrent ventricular tachycardias (VTs). However, at least in part, procedural and clinical outcomes are limited by challenges in generating an adequate lesion size in the ventricular myocardium. We investigated procedural and clinical outcomes of VT ablation using a novel 'large-footprint' catheter that allows the creation of larger lesions either by radiofrequency (RF) or by pulsed field (PF) energy.
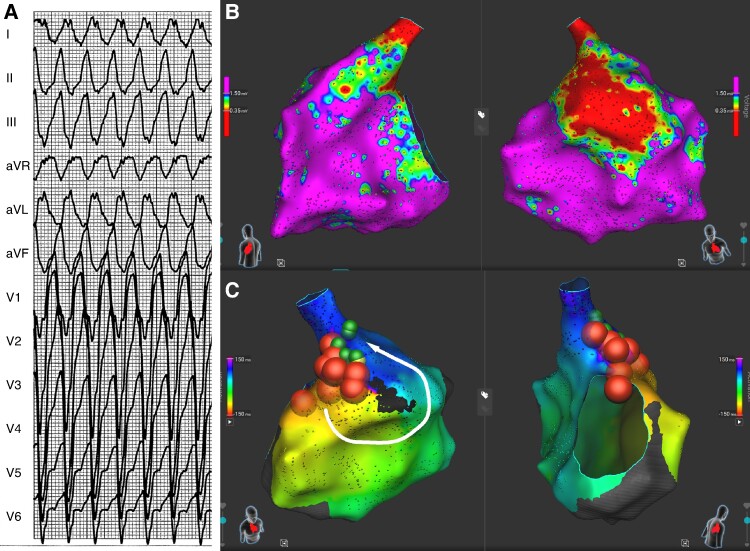
Methods and results: In prospectively collected case series, we describe our initial experience with VT ablation using a lattice-tip, dual-energy catheter (Sphere-9, Medtronic), and a compatible proprietary electroanatomical mapping system (Affera, Medtronic). The study population consisted of 18 patients (aged 55 ± 15 years, one woman, structural heart disease: 94%, ischaemic heart disease: 56%, left ventricular ejection fraction: 34 ± 10%, electrical storm: 22%) with recurrent sustained VTs and ≥1 previously failed endocardial RF ablation with conventional irrigated-tip catheter in 66% of patients. On average, 12 ± 7 RF and 8 ± 9 PF applications were delivered per patient. In three-fourths of patients undergoing percutaneous epicardial ablation, spasms in coronary angiography were observed after PF applications. All resolved after intracoronary administration of nitrates. No acute phrenic nerve palsy was noted. One patient suffered from a stroke that resolved without sequelae. Post-ablation non-inducibility of VT was achieved in 89% of patients. Ventricular-arrhythmia-free survival at three months was 78%.
Conclusion: VT ablation using a dual-energy lattice-tip catheter and a novel electroanatomical mapping system is feasible. It allows rapid mapping and effective substrate modification with good outcomes during short-term follow-up.
Keywords: Catheter ablation; Pulsed field; Radiofrequency ablation; Ventricular tachycardia.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: J.K. reports personal fees from Biosense Webster, Boston Scientific, GE Healthcare, Medtronic, and St. Jude Medical (Abbott) for participation in scientific advisory boards and has received speaker honoraria from Biosense Webster, Biotronik, Boston Scientific, Medtronic, ProMed CS, St. Jude Medical (Abbott), and Viatris. P.P. has received speaker honoraria from St. Jude Medical (Abbott) and Medtronic and has served as a consultant for Biotronik and Boston Scientific. V.N. is an employee of Medtronic. The remaining authors have no disclosures to declare.
Figures





References
-
- Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;40:3997–4126. - PubMed
-
- Ravi V, Poudyal A, Khanal S, Khalil C, Vij A, Sanders D et al. A systematic review and meta-analysis comparing radiofrequency catheter ablation with medical therapy for ventricular tachycardia in patients with ischemic and non-ischemic cardiomyopathies. J Interv Card Electrophysiol 2023;66:161–75. - PubMed
-
- Della Bella P, Baratto F, Vergara P, Bertocchi P, Santamaria M, Notarstefano P et al. Does timing of ventricular tachycardia ablation affect prognosis in patients with an implantable cardioverter defibrillator? Results from the multicenter randomized PARTITA trial. Circulation 2022;145:1829–38. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
