

Efficacy of mechanical against manual method in cardiopulmonary resuscitation for out‑of‑hospital cardiac arrest: A meta‑analysis
- PMID: 39478734
- PMCID: PMC11523225
- DOI: 10.3892/etm.2024.12748
Efficacy of mechanical against manual method in cardiopulmonary resuscitation for out‑of‑hospital cardiac arrest: A meta‑analysis
Abstract
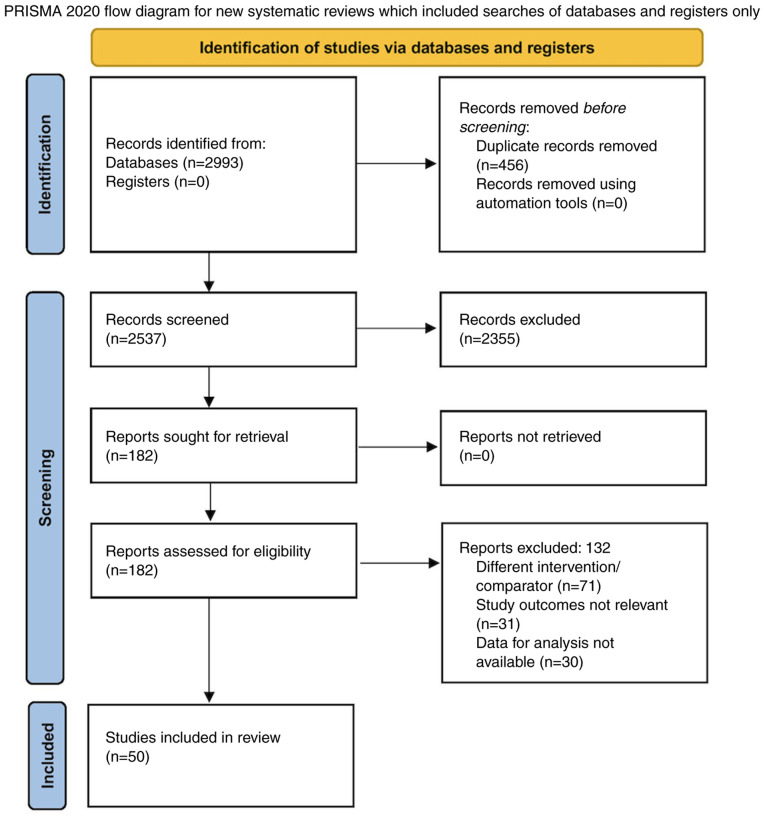
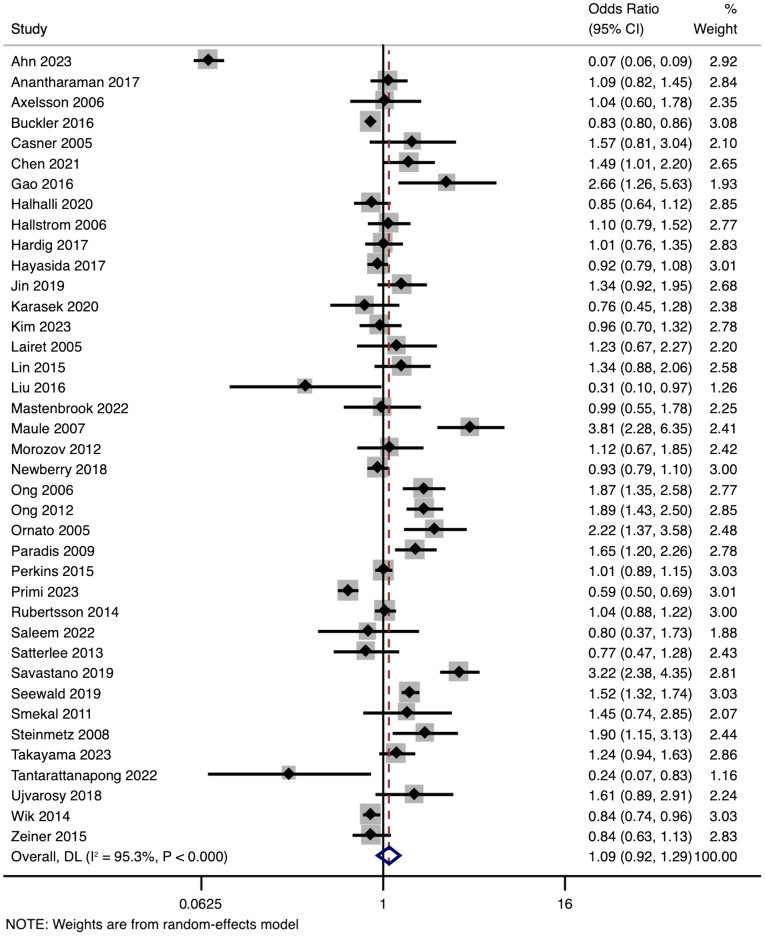
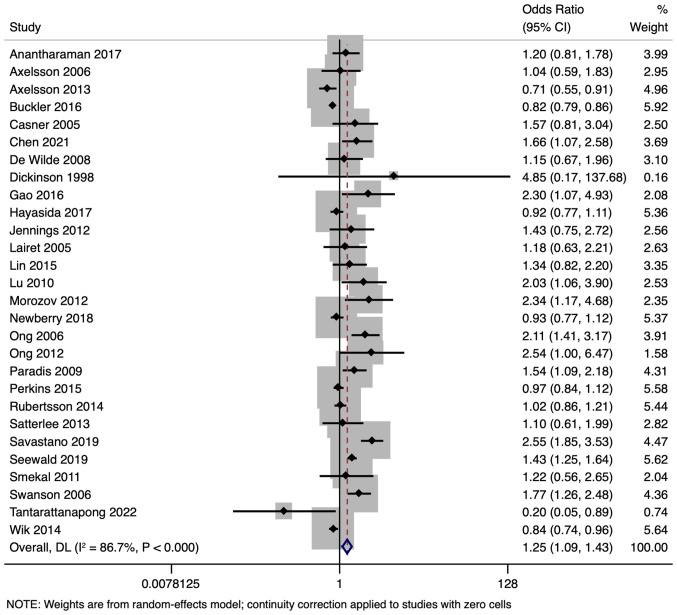
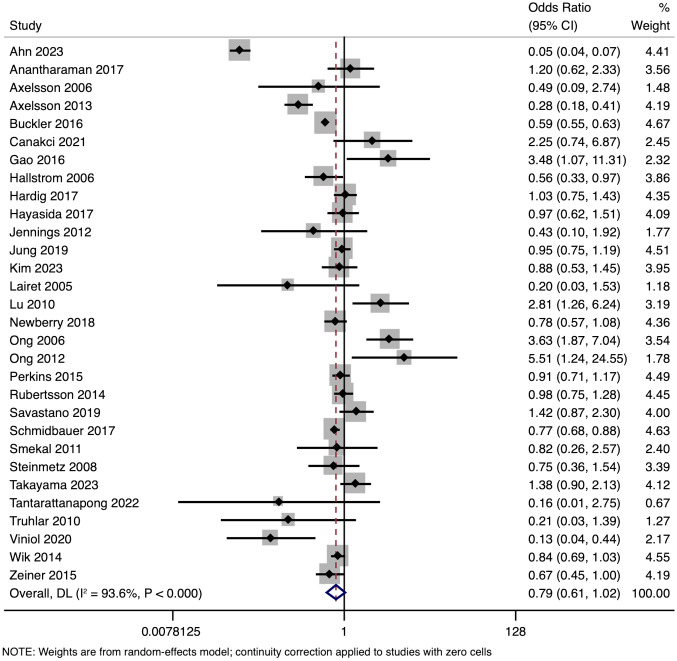
Out-of-hospital cardiac arrest (OHCA) remains a leading cause of mortality worldwide, with the efficacy of cardiopulmonary resuscitation (CPR) methods playing a crucial role in patient outcomes. The present study aimed to compare the effectiveness of mechanical and manual CPR in OHCA, focusing on three outcomes: Return of spontaneous circulation (ROSC), survival to admission and survival till discharge. A comprehensive meta-analysis was conducted, incorporating 39 studies for ROSC, 28 for survival to admission, and 30 for survival till discharge, totalling 144,430, 130,499 and 162,088 participants, respectively. The quality of evidence was evaluated using the GRADE approach, assessing risk of bias, inconsistency, indirectness, imprecision and publication bias. Statistical analysis included pooled odds ratios (ORs) with 95% confidence intervals (CIs) and sensitivity analyses. For ROSC, the pooled OR was 1.09 (95% CI: 0.92-1.29), demonstrating no significant difference between mechanical and manual CPR. Survival to admission favoured mechanical CPR with a pooled OR of 1.25 (95% CI: 1.09-1.43). No conclusive difference was found for survival till discharge, with a pooled OR of 0.79 (95% CI: 0.61-1.02). Substantial heterogeneity was observed across outcomes. Evidence of potential publication bias was noted, particularly in the survival to admission outcome. The overall quality of evidence was graded as very low, mainly due to high heterogeneity and indirectness of evidence. The study suggests that mechanical CPR may improve short-term outcomes such as survival to admission in patients with OHCA but does not demonstrate a significant long-term survival benefit over manual CPR.
Keywords: cardiopulmonary resuscitation; meta-analysis; out of hospital cardiac arrest.
Copyright: © 2024 Zhu and Fu.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Committee on the Treatment of Cardiac Arrest; Current Status and Future Directions; Board on Health Sciences Policy and Institute of Medicine: Strategies to Improve Cardiac Arrest Survival: A Time to Act. Graham R, McCoy MA and Schultz AM (eds). National Academies Press, Washington, DC, 2015. - PubMed
-
- Goyal A, Sciammarella JC, Cusick AS, Patel PH. Cardiopul-monary resuscitation. In: StatPearls [Internet]. StatPearls Publishing, Treasure Island, FL, 2024.
LinkOut - more resources
Full Text Sources