

Optimising availability and geographical accessibility to emergency obstetric care within a sub-national social health insurance scheme in Nigeria
- PMID: 39478850
- PMCID: PMC11521965
- DOI: 10.3389/frhs.2024.1460580
Optimising availability and geographical accessibility to emergency obstetric care within a sub-national social health insurance scheme in Nigeria
Abstract
Introduction: Health insurance is a key instrument for a health system on its path to achieving universal health coverage (UHC) and protects individuals from catastrophic health expenditures, especially in health emergencies. However, there are other dimensions to care access beyond financial accessibility. In this study, we assess the geographical accessibility of comprehensive emergency obstetric care (CEmOC) within the Lagos State Health Insurance Scheme.
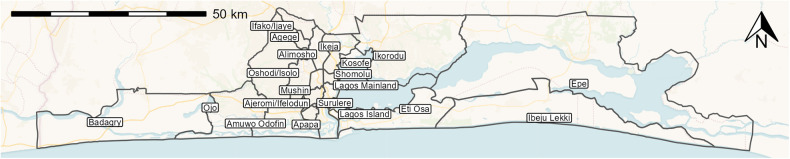
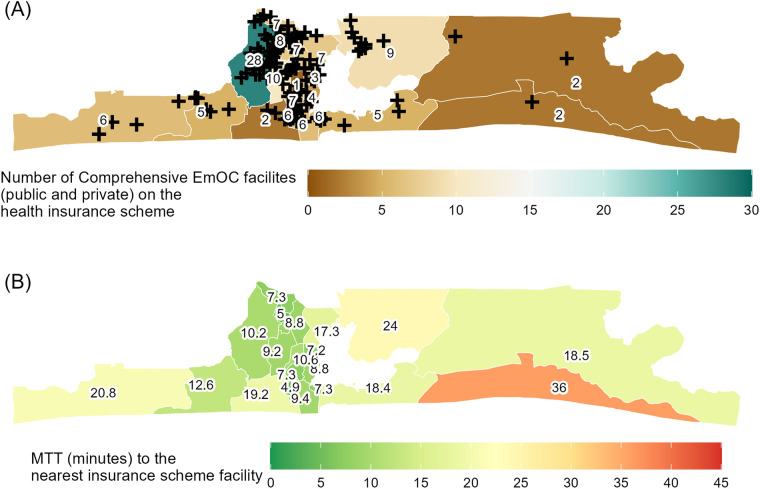
Methods: We geocoded functional public and private CEmOC facilities, established facilities registered on the insurance panel as of December 2022, and assembled population distribution for women of childbearing age. We used Google Maps Platform's internal directions application programming interface to obtain driving times to facilities. State- and local government area (LGA)-level median travel time (MTT) and a number of CEmOC facilities reachable within 30 min were obtained for peak travel hours.
Results: Across Lagos State, MTT to the nearest public CEmOC was 25 min, reduced to 17 min with private facilities added to the insurance panel. MTT to the nearest public facility in LGAs ranged from 9 min (Lagos Island) to 51 min (Ojo) (median = 25 min). With private facilities added, MTT ranged from 5 min (Agege and Ajeromi-Ifelodun) to 36 min (Ibeju-Lekki) (median = 13 min). On average, no public CEmOC facility was reachable within 30 min of driving for women living in 6 of 20 LGAs. With private facilities included in the scheme, reachable facilities within 30 min remained zero in one LGA (Ibeju-Lekki).
Conclusions: Our innovative approach offers policy-relevant evidence to optimise insurance coverage, support efforts in advancing UHC, ensure coverage for CEmOC, and improve health system performance.
Keywords: emergency obstetric care; geographical accessibility; health insurance; maternal health; universal health coverage.
© 2024 Banke-Thomas, Olubodun, Olaniran, Wong, Shah, Achugo and Ogunyemi.
Conflict of interest statement
YS is an employee of Google LLC, which developed the Google Maps Platform. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declare that this study received funding from Google. Technical team members from the funding organisation were involved in extracting the travel time estimates and drafting the description of the travel time estimation in the manuscript. However, the funder was not involved in the study conceptualisation, study design, analysis, interpretation of data, or the decision to submit it for publication.
Figures
References
-
- WHO. Universal Health Coverage. Health topics; (2020). Available online at: https://www.who.int/health-topics/universal-health-coverage#tab=tab_1 (cited November 20, 2020)
-
- United Nations. Transforming our world: the 2030 Agenda for Sustainable Development. In: Resolution Adopted by the General Assembly on 25 September 2015. New York: United Nations General Assembly; (2015). p. 1–7.
-
- Ghosh S. Catastrophic payments and impoverishment due to out-of-pocket health spending. Econ Polit Wkly. (2011) 46(47):64–70.
Associated data
LinkOut - more resources
Full Text Sources